Serum Cholesterol levels
Discussion


Wicker Man said:
Not so!
And whilst most busy GPs might try to opt for a quiet life, if you look at the link I posted above, you will see some very prominent doctors:
Leading Doctors Reject Latest Statin Guidance From The National Institute for Health and Care
Excellence
An open letter has been sent to the chair of NICE and the secretary of state for health, Jeremy Hunt,
from leading doctors in primary care, secondary care and academia. They reject the recent draft
guidance from NICE to reduce the threshold for prescribing statins to those with a 10% risk of
cardiovascular disease (potentially treating an additional five million healthy individuals).
The letter is signed by a number of leading figures in health including the president of the Royal
College of Physicians, Sir Richard Thompson, Professor Clare Gerada, Past Chair of the Royal College of
General Practitioners and Professor Simon Capewell, Clinical Epidemiologist at the University of
Liverpool.
Other signatories include Professor David Haslam, Chair Of The National Obesity Forum, GP Dr
Malcolm Kendrick, London Cardiologist Dr Aseem Malhotra and Professor David Newman, Emergency
Medicine physician and Director of clinical research and Mount Sinai School of Medicine, New York.
They address six major concerns and call on NICE to refrain from any final recommendations on
reducing the threshold for statin guidance until these are fully addressed.
These six key areas are:
1. The medicalization of millions of healthy individuals
2. Conflicting levels of adverse events
3. Hidden data
4. Industry bias
5. Loss of professional
Those links are 10 years old- are they still saying the same thing or have 10 years of data changed things?And whilst most busy GPs might try to opt for a quiet life, if you look at the link I posted above, you will see some very prominent doctors:
Leading Doctors Reject Latest Statin Guidance From The National Institute for Health and Care
Excellence
An open letter has been sent to the chair of NICE and the secretary of state for health, Jeremy Hunt,
from leading doctors in primary care, secondary care and academia. They reject the recent draft
guidance from NICE to reduce the threshold for prescribing statins to those with a 10% risk of
cardiovascular disease (potentially treating an additional five million healthy individuals).
The letter is signed by a number of leading figures in health including the president of the Royal
College of Physicians, Sir Richard Thompson, Professor Clare Gerada, Past Chair of the Royal College of
General Practitioners and Professor Simon Capewell, Clinical Epidemiologist at the University of
Liverpool.
Other signatories include Professor David Haslam, Chair Of The National Obesity Forum, GP Dr
Malcolm Kendrick, London Cardiologist Dr Aseem Malhotra and Professor David Newman, Emergency
Medicine physician and Director of clinical research and Mount Sinai School of Medicine, New York.
They address six major concerns and call on NICE to refrain from any final recommendations on
reducing the threshold for statin guidance until these are fully addressed.
These six key areas are:
1. The medicalization of millions of healthy individuals
2. Conflicting levels of adverse events
3. Hidden data
4. Industry bias
5. Loss of professional
Wicker Man said:
I’ve not heard of Ezetimbe before but I see it’s another weapon in the war on cholesterol. That’s the whole premise that many reputable doctors and scientists question challenge! (At least those that have read the early Framingham trial papers etc past the abstract.)
Cholesterol is made in our amazing livers, is vital to every part of the body, our brains more than most. I want my liver to function normally and not be poisoned by some nasty pharmaceutical concoction based on bad science.
Agreed, but for the small number of people with hypercholesterolemia is quite important to control cholesterol.Cholesterol is made in our amazing livers, is vital to every part of the body, our brains more than most. I want my liver to function normally and not be poisoned by some nasty pharmaceutical concoction based on bad science.
If money were no object I would go for a PCSK9 based drug like alirocumab
craig1912 said:
Those links are 10 years old- are they still saying the same thing or have 10 years of data changed things?
Here's a recent blog post (Dec '23) from Dr Kendrick (one of the authors mentioned above): https://drmalcolmkendrick.org/2023/12/10/very-high...So, still the same: cholesterol is not the root cause of CVD.
From the linked blog post:
said:
The prediction was that the group with the highest LDL-cholesterol levels should have considerably more plaques and/or calcification in their arteries.
They did not find any statistically significant difference between the two groups. So, it did not appear to matter if you had ‘super high LDL’ or ‘normal” LDL cholesterol. In fact, the trend was that the people with the high cholesterol had less plaque in their arteries.
For there to be causation, you'd at least expect some correlation.They did not find any statistically significant difference between the two groups. So, it did not appear to matter if you had ‘super high LDL’ or ‘normal” LDL cholesterol. In fact, the trend was that the people with the high cholesterol had less plaque in their arteries.
As for cholesterol v all-cause mortality (blue line below), deliberately lowering your cholesterol levels with drugs would appear to be a little risky:
The main benefit of statins in combatting CVD appears to be through improving parameters associated with endothelial function, eg by preventing hypoxia-induced downregulation of eNOS in endothelial cells.
Dr Kendrick has long argued that it's the loss of endothelial function that is the root cause of so much CVD. Cholesterol is used to repair endothelial damage and thus the more dysfunction, the more plaque will accumulate from repairs. As these deposits slough off then you risk blockages. The fix? Preventing the damage in the first place (for which you don't need statins), not the repair mechanism.
Blaming cholesterol for CVD is like blaming firefighters for house fires.
It’s fascinating the physchology of this
100k cardiologists vs a GP’s blog post (which is mostly a forwarded email describing an unreleased metaanalysis!)
And you pick the one who tells you to keep eating sausages!
Also the NHS is moving away from LDL. There are other markers (most cheaply non HDL) that are more predictive.
End of day nobody is saying excercise and diet isn’t best for most healthy people. (Some with abnormalities may need meds regardless)
I think most people are much less healthy than they think however.
100k cardiologists vs a GP’s blog post (which is mostly a forwarded email describing an unreleased metaanalysis!)
And you pick the one who tells you to keep eating sausages!
Also the NHS is moving away from LDL. There are other markers (most cheaply non HDL) that are more predictive.
End of day nobody is saying excercise and diet isn’t best for most healthy people. (Some with abnormalities may need meds regardless)
I think most people are much less healthy than they think however.
Edited by lizardbrain on Saturday 20th April 11:08
lizardbrain said:
It’s fascinating the physchology of this
100k cardiologists vs a GP’s blog post (which is mostly a forwarded email!)
And you pick the one who tells you to keep eating sausages!
Sorry, what's your point? 100k cardiologists vs a GP’s blog post (which is mostly a forwarded email!)
And you pick the one who tells you to keep eating sausages!
The question was "... are they still saying the same after 10 years". I picked one of the names, linked to a recent communication to demonstrate that yes, at least one is.
Where do sausages even come into it?
Fair enough. I see the guy had a libel case recently though not sure what the result it
as for the point, I think it was pretty clear. Interesting the weight people place in an outlier GP when their position affirms their own position
As for cause of cvd. That would be living. I don’t think anyone is disputing lifestyle is best for prevent cvd. That would sadly include not eating sausages.
End of day it’s a complex area and i would advise to ask a cardiologist, and imo they can be trusted more than a gp to look past the population level stuff into your specific case. An appointment will cost 150-200
as for the point, I think it was pretty clear. Interesting the weight people place in an outlier GP when their position affirms their own position
As for cause of cvd. That would be living. I don’t think anyone is disputing lifestyle is best for prevent cvd. That would sadly include not eating sausages.
End of day it’s a complex area and i would advise to ask a cardiologist, and imo they can be trusted more than a gp to look past the population level stuff into your specific case. An appointment will cost 150-200
Edited by lizardbrain on Saturday 20th April 11:55
lizardbrain said:
Fair enough. I see the guy had a libel case recently though not sure what the result it
as for the point, I think it was pretty clear. Interesting the weight people place in an outlier GP when their position affirms their own lifestyle choices. Despite every cardiology org in the world saying the opposite.
Quite interesting
I could reference others, but it's a forum post, not a medical paper. Your expectations as to the completeness of associated reference materials seem somewhat excessive given the medium.as for the point, I think it was pretty clear. Interesting the weight people place in an outlier GP when their position affirms their own lifestyle choices. Despite every cardiology org in the world saying the opposite.
Quite interesting
Since you've mentioned the libel case, you'll at least recognise Zoe Harcombe as co-claimant in their libel case against The Mail Online and The Mail on Sunday. Have you read her PhD thesis? You should. It's very good.
jagnet said:
I could reference others, but it's a forum post, not a medical paper. Your expectations as to the completeness of associated reference materials seem somewhat excessive given the medium.
Since you've mentioned the libel case, you'll at least recognise Zoe Harcombe as co-claimant in their libel case against The Mail Online and The Mail on Sunday. Have you read her PhD thesis? You should. It's very good.
No I havn’t read it as I’m not medically trained so would likely misinterpret the context and the weight of the findings. Since you've mentioned the libel case, you'll at least recognise Zoe Harcombe as co-claimant in their libel case against The Mail Online and The Mail on Sunday. Have you read her PhD thesis? You should. It's very good.
So fundamentally I reject the point of referencing stuff on a forum at all. Vs talking to a doctor ideally a cardiologist about your specific individual case
Referencing health guidelines is a bit different as these are the guidelines that guide our treatment and care
lizardbrain said:
..vs talking to a doctor
People should listen to their doctors. If anyone's going to know about diet and nutrition it's going to be a doctor. Some of them have anything up to a whole 24 hours of nutrition training during medical school https://www.bbc.co.uk/news/health-43504125Rumour has it that some even know the difference between cholesterol and lipoproteins.
jagnet said:
People should listen to their doctors. If anyone's going to know about diet and nutrition it's going to be a doctor. Some of them have anything up to a whole 24 hours of nutrition training during medical school https://www.bbc.co.uk/news/health-43504125
Rumour has it that some even know the difference between cholesterol and lipoproteins.
Doctors in my experience rigidly follow guidelines. And in same cases will follow guidelines even if they are aware of more recent research. Rumour has it that some even know the difference between cholesterol and lipoproteins.
However the guidelines have a lot of weight and expertise behind them. And as far as I know it’s the guidelines not the doctors you consider incorrect?
lizardbrain said:
However the guidelines have a lot of weight and expertise behind them.
Weight, yes. The expertise behind the nutritional guidelines, however, was more political than medical: https://www.theguardian.com/society/2016/apr/07/th...My story is that I believe Statins do reduce cholesterol, but I also believe they are handed out like sweets by GPs. It's a pretty heavy family of drugs.
My recent experience is that my total Cholesterol was recorded as 5.9 so my CVD risk score increased to over 10%. I then received an automatic text from my GP asking me to attend so we could discuss going onto Statins.
That's when I decided to carry out some in-depth research into CVD, Cholesterol and Statins. I didn't realise before that it was such a controversial topic.
I've now had a private ApoB blood test which seems to be the generally accepted 'most accurate' risk identifier. The NHS can't afford to do it to the population at risk, so we're left with a half arsed standard measure of LDL and non HDL.
I'm currently investigating how to get my Lp(a) tested as this will tell me my hereditary risk factor. This test doesn't seem to be straight forward, but at least it only needs to be done once in your life.
So the journey continues, but I won't be going onto Statins until I have the complete picture and I can see my personal risk level.
My recent experience is that my total Cholesterol was recorded as 5.9 so my CVD risk score increased to over 10%. I then received an automatic text from my GP asking me to attend so we could discuss going onto Statins.
That's when I decided to carry out some in-depth research into CVD, Cholesterol and Statins. I didn't realise before that it was such a controversial topic.
I've now had a private ApoB blood test which seems to be the generally accepted 'most accurate' risk identifier. The NHS can't afford to do it to the population at risk, so we're left with a half arsed standard measure of LDL and non HDL.
I'm currently investigating how to get my Lp(a) tested as this will tell me my hereditary risk factor. This test doesn't seem to be straight forward, but at least it only needs to be done once in your life.
So the journey continues, but I won't be going onto Statins until I have the complete picture and I can see my personal risk level.
Having read through here today, it's clear to me that I need to do some research.
The details your are discussing are very interesting and helpful and much appreciated.
About 15 years ago a blood test identified my cholesterol score at 9.1, for which my Doctor immediately put me on statins.
As my work had me flying all over place every month, in different time zones, I failed to maintain a schedule with my meds., and so the Doctor stopped them.
By this time, I had started taking Omega 3 and Flax seed oil capsules, and, not forgetting, red wine.
My Doctor had me retested with the result being 5.9.
Last week I had new results at 5.3 and am investigating these details, family risk etc.
PS. about 8 years ago I ended up spending a week in a German hospital with chest pains.
During the initial examination, the Doctor asked if I drank, to which I responded, "Yes, red wine". His response was, "Ah good, good man, good man, nothing wrong with that".
My kind of Doctor.
The details your are discussing are very interesting and helpful and much appreciated.
About 15 years ago a blood test identified my cholesterol score at 9.1, for which my Doctor immediately put me on statins.
As my work had me flying all over place every month, in different time zones, I failed to maintain a schedule with my meds., and so the Doctor stopped them.
By this time, I had started taking Omega 3 and Flax seed oil capsules, and, not forgetting, red wine.
My Doctor had me retested with the result being 5.9.
Last week I had new results at 5.3 and am investigating these details, family risk etc.
PS. about 8 years ago I ended up spending a week in a German hospital with chest pains.
During the initial examination, the Doctor asked if I drank, to which I responded, "Yes, red wine". His response was, "Ah good, good man, good man, nothing wrong with that".
My kind of Doctor.
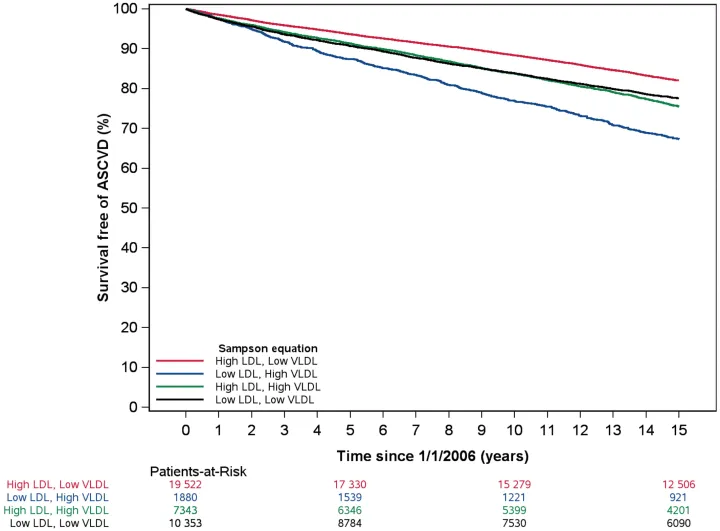
Interesting results from a new JAHA paper published this month - seems appropriate for this thread:
https://doi.org/10.1161/JAHA.123.031878
Imagine how much worse it would be if they hadn't had their statins [insert appropriate emoji]
https://doi.org/10.1161/JAHA.123.031878
Seehusen et al said:
Those with discordantly high LDL‐C and low VLDL‐C experienced the lowest atherosclerotic cardiovascular disease (ASCVD) rate (7.7 per 1000 person‐years); conversely, the group with discordantly low LDL‐C and high VLDL‐C experienced the highest crude ASCVD rate (16.9 per 1000 person‐years).
The low LDL-C / high VLDL-C cohort is notable for having the highest incidence of diabetes, high blood pressure, high triglyceride levels, high statin use, low total cholesterol, highest risk of CVD.Imagine how much worse it would be if they hadn't had their statins [insert appropriate emoji]
jagnet said:
Imagine how much worse it would be if they hadn't had their statins [insert appropriate emoji]
I know from experience that doctors are very reluctant to prescribe statins to someone with higher LDL who otherwise seems healthy. Especially if there is room to improve diet and exercise.
So I remain confused what your point is really.
You never did answer my question. Do you agree statins are net helpful for those with proven CVD or highly abmormal lipids with can't be controlled with lifestyle?
lizardbrain said:
So I remain confused what your point is really.
That attempting to prolong life by artificially lowering cholesterol levels is not a great idea, because cholesterol is not the root cause of CVD. It is, however, vital to life.lizardbrain said:
You never did answer my question. Do you agree statins are net helpful for those with proven CVD or highly abmormal lipids with can't be controlled with lifestyle?
For men, over 55, that have already had a CVD-related blip then there would appear to be a slight reduction in further CVD-related incidents from taking statins - off the top of my head it's something like 1 fewer incident (of all types, not just fatal) for every 50 men treated.This slight benefit would not appear to be related to statins' primary function of lowering cholesterol, but rather through improvements to endothethial function.
The study above suggests that even that could be overstating their benefits in the long-term.
jagnet said:
For men, over 55, that have already had a CVD-related blip then there would appear to be a slight reduction in further CVD-related incidents from taking statins - off the top of my head it's something like 1 fewer incident (of all types, not just fatal) for every 50 men treated.
This slight benefit would not appear to be related to statins' primary function of lowering cholesterol, but rather through improvements to endothethial function.
The study above suggests that even that could be overstating their benefits in the long-term.
Your definition of 'slight' is dubious. If there is 2 incidents for every 50 men without treatment, and 1 incidence for every 50 men with treatment. Then taking the statin confers a 50% reduction in risk for the individual. This slight benefit would not appear to be related to statins' primary function of lowering cholesterol, but rather through improvements to endothethial function.
The study above suggests that even that could be overstating their benefits in the long-term.
The mechanism by which statins work to reduce events is moot.
Non HDL is highly predictive
The study states no such thing IMO. You don't seem qualified to interpret this data.
Salt is vital to life too. doesn't mean we should eat it by
Gassing Station | Health Matters | Top of Page | What's New | My Stuff