Grassing up a Covid **** taker.
Discussion


Phil. said:
There is so much opinion here which disagrees with the evidence that I can’t be arsed to pick it out. Try posting the same message here and I’m sure you’ll get lots of responses:
https://www.pistonheads.com/gassing/topic.asp?h=0&...
https://www.pistonheads.com/gassing/topic.asp?h=0&...

Phil. said:
Evanivitch said:
So weird that rather than link to the data, you link to a Twitter link of a paywall article. How odd.
Not as odd as your replies Give it a couple of days and the article will be available for viewing by everyone and/or other press will publish similar articles. Or take the effort to research the increasing number of home deaths during COVID interventions this year because they is a lot of information about. Or continue making dumb responses to my posts just cos’ you really dislike me on PH

Chromegrill said:
Phil. said:
There is so much opinion here which disagrees with the evidence that I can’t be arsed to pick it out. Try posting the same message here and I’m sure you’ll get lots of responses:
https://www.pistonheads.com/gassing/topic.asp?h=0&...
Otherwise known as, please don't confuse me with the facts as I've already made up my mind. Did you actually bother to read anything that I posted?https://www.pistonheads.com/gassing/topic.asp?h=0&...
Evanivitch said:
Phil. said:
Evanivitch said:
So weird that rather than link to the data, you link to a Twitter link of a paywall article. How odd.
Not as odd as your replies Give it a couple of days and the article will be available for viewing by everyone and/or other press will publish similar articles. Or take the effort to research the increasing number of home deaths during COVID interventions this year because they is a lot of information about. Or continue making dumb responses to my posts just cos’ you really dislike me on PH
I provided the source of the data in the original post but being the idiot you are you just want to argue the toss about nothing for as long as you possibly can. I suggest you get yourself out to the supermarket and load up on bog roll before your beloved circuit breaker comes in to force, something I know you have been longing for. I expect you like sitting on your arse all day so you will have a great next 2 weeks spouting s te on PH. Enjoy.
te on PH. Enjoy. Killboy said:
Phil. said:
Killboy said:
Phil. said:
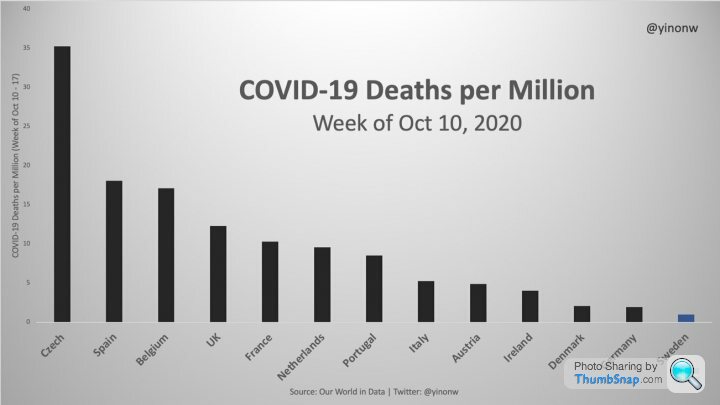
Source of data?
It’s not a random Twitter user 
Not enough 3d effect on the graph, and comic sans fonts for you?
R Mutt said:
Chromegrill said:
I can't understand why everyone seems to want to be like Sweden when their cumulative mortality rates per capita are the fifth highest in Europe. It's embarrassing when you think of the amount of free space compared to many countries and the natural distancing possible in Swedish culture which simply does not translate into anything possible in the UK. I'm more interested in understanding why low and middle income countries like mongolia, Ghana, Taiwan or Vietnam have managed to contain the virus from the outset and have suffered little economic hardship in comparison to us. In short, countries with a vigorous response from the beginning and rigorous lockdown as soon as it was needed have done much better economically on the whole than those like the UK that have attempted to ride it out, then slammed the brakes on when it was too late. No-one wants another lockdown, and those making the decision are acutely aware of the harms to jobs, mental wellbeing, education and the economy. So why would they even consider it again?
There has been some chatter on this thread about intensive care beds. I'd just like to point out that France, which is about a month ahead of us in terms of COVID-19 rates, currently has 2000 ICU beds occupied by patients with COVID-19. The UK has around 4000 ICU beds in total, most of which are currently filled with patients who have conditions other than COVID-19 so there are very few "spare" ICU beds available. Just because they aren't half full yet with patients with COVID-19 doesn't mean we can afford to be complacent, and I have to point out that the numbers of patients in our ICU beds is growing exponentially. That doesn't just mean that the number every day is bigger than the number the previous day. It means in layman's terms, that the difference between yesterday's count and today's is bigger than the day before yesterday's and today's counts. That is incredibly worrying for those of us working in the field, given that the only intervention proven to curb numbers is the full lockdown we had in March. The "R" number fell overnight when it was introduced and the mortality began falling a fortnight later, exactly as expected from what we know of this infection.
You may ask why people don't seem to be dying from COVID in large numbers at present in the UK. Well the number of patients who die from COVID is proportional to the number of patients admitted with COVID, which is proportional to the number of people infected across the community. And the number of deaths is growing exponentially, a few weeks behind the same rate of growth in cases and starting from very low numbers so it will take a while to see the changes. But we can't undo the infections that have already occurred, and we know that a (thankfully fairly small) proportion of them will go on to become very sick, and some of them will die from this. When you have unrestricted spread of infectious, as we have seen in recent weeks, a proportion of them will be admitted to hospital in due course. And some of those who are critically sick may be in hospital a few weeks before they die. We know this because it's what happened in March and it's the same virus. It hasn't mutated and we aren't massively better at treating it now than we were before. True we have learnt a lot over the past few months and around a quarter of the patients who previously died in intensive care might now survive with improvements to the way we use steroids and breathing support but none of the widely-touted drugs like hydroxychloroquine or remdesivir have proven, after clinical rigorous trials, to have any impact whatsoever on mortality. Put bluntly, they don't work on the COVID-19 coronavirus.
Oh and don't think that just because winter is always a busy time that the doctors and nurses in ICU are bleating about something that's no different than usual. Fewer staff are available than usual this year (because at any point we have colleagues who are isolating at home with COVID, isolating at home because a family member or other close contact of them has COVID or they are staying at home because their children have been sent home from school because a classmate caught it). So for starters there is the same amount of work to do as usual but fewer staff to do it. And it's psychologically hard when you recognise some of the patients in intensive care as being your own colleagues. Yep, happened in March, don't want to repeat it again.
Then we have all the additional precautions necessary to avoid the healthcare workforce becoming infected, or infecting our patients. Like physical spacing so there isn't as much room for as many beds as usual. Like everything taking so much longer when you have patients in ICU with COVID because of all the additional PPE you have to change in and out of. Like knowing that because surgeons are still trying to play catch up with surgery that had to be delayed from earlier in the year we are juggling patients who need critical care beds after surgery with the possibility those beds may not be available for very much longer if they end up being taken up with patients who require ventilation due to COVID. And if things get really bad and we have to take over the operating theatres again in some hospitals, as we did back in March, in order to make use of their ventilators, then obviously some people who need surgery will have further delays. Don't underestimate how complicated and exhausting it is this year compared to the annual winter bugs festival that comes along every year in the autumn.
I hope it doesn't get to that point, and we still have time to prevent it doing so but infection rates are getting worryingly high. Belgium has just admitted they are unable to cope any longer and we have a small window of opportunity to seize back control and avoid going down the same route. COVID-19 is not flu - it's something like ten times more deadly than flu, and a lot of people can all fall very sick at the same time if it's allowed to get out of hand. As a society we can choose which way we want to go with this, but we need to accept that it won't be brought under control if if half the population want tighter restrictions and the other half still think it's just a hoax. Which half are you in?
People are still ignoring the fact that the Swedish figures aren't great and that Swedes have been following social distancing and other recommendedmeasures. It was the same early on with the praise of S. Korea. Except people liked their figures rather than the actual response which was to track and trace you down to your home and make you quarantine. While people here saying what a mess we've made of it are refusing to write their real name down in a pub.There has been some chatter on this thread about intensive care beds. I'd just like to point out that France, which is about a month ahead of us in terms of COVID-19 rates, currently has 2000 ICU beds occupied by patients with COVID-19. The UK has around 4000 ICU beds in total, most of which are currently filled with patients who have conditions other than COVID-19 so there are very few "spare" ICU beds available. Just because they aren't half full yet with patients with COVID-19 doesn't mean we can afford to be complacent, and I have to point out that the numbers of patients in our ICU beds is growing exponentially. That doesn't just mean that the number every day is bigger than the number the previous day. It means in layman's terms, that the difference between yesterday's count and today's is bigger than the day before yesterday's and today's counts. That is incredibly worrying for those of us working in the field, given that the only intervention proven to curb numbers is the full lockdown we had in March. The "R" number fell overnight when it was introduced and the mortality began falling a fortnight later, exactly as expected from what we know of this infection.
You may ask why people don't seem to be dying from COVID in large numbers at present in the UK. Well the number of patients who die from COVID is proportional to the number of patients admitted with COVID, which is proportional to the number of people infected across the community. And the number of deaths is growing exponentially, a few weeks behind the same rate of growth in cases and starting from very low numbers so it will take a while to see the changes. But we can't undo the infections that have already occurred, and we know that a (thankfully fairly small) proportion of them will go on to become very sick, and some of them will die from this. When you have unrestricted spread of infectious, as we have seen in recent weeks, a proportion of them will be admitted to hospital in due course. And some of those who are critically sick may be in hospital a few weeks before they die. We know this because it's what happened in March and it's the same virus. It hasn't mutated and we aren't massively better at treating it now than we were before. True we have learnt a lot over the past few months and around a quarter of the patients who previously died in intensive care might now survive with improvements to the way we use steroids and breathing support but none of the widely-touted drugs like hydroxychloroquine or remdesivir have proven, after clinical rigorous trials, to have any impact whatsoever on mortality. Put bluntly, they don't work on the COVID-19 coronavirus.
Oh and don't think that just because winter is always a busy time that the doctors and nurses in ICU are bleating about something that's no different than usual. Fewer staff are available than usual this year (because at any point we have colleagues who are isolating at home with COVID, isolating at home because a family member or other close contact of them has COVID or they are staying at home because their children have been sent home from school because a classmate caught it). So for starters there is the same amount of work to do as usual but fewer staff to do it. And it's psychologically hard when you recognise some of the patients in intensive care as being your own colleagues. Yep, happened in March, don't want to repeat it again.
Then we have all the additional precautions necessary to avoid the healthcare workforce becoming infected, or infecting our patients. Like physical spacing so there isn't as much room for as many beds as usual. Like everything taking so much longer when you have patients in ICU with COVID because of all the additional PPE you have to change in and out of. Like knowing that because surgeons are still trying to play catch up with surgery that had to be delayed from earlier in the year we are juggling patients who need critical care beds after surgery with the possibility those beds may not be available for very much longer if they end up being taken up with patients who require ventilation due to COVID. And if things get really bad and we have to take over the operating theatres again in some hospitals, as we did back in March, in order to make use of their ventilators, then obviously some people who need surgery will have further delays. Don't underestimate how complicated and exhausting it is this year compared to the annual winter bugs festival that comes along every year in the autumn.
I hope it doesn't get to that point, and we still have time to prevent it doing so but infection rates are getting worryingly high. Belgium has just admitted they are unable to cope any longer and we have a small window of opportunity to seize back control and avoid going down the same route. COVID-19 is not flu - it's something like ten times more deadly than flu, and a lot of people can all fall very sick at the same time if it's allowed to get out of hand. As a society we can choose which way we want to go with this, but we need to accept that it won't be brought under control if if half the population want tighter restrictions and the other half still think it's just a hoax. Which half are you in?
Phil. said:
otolith said:
Phil. said:
otolith said:
You keep posting the same link without any explanation expecting others to interpret it for you. Care to explain what point you keep trying to make with this public information link? It lists the measures and restrictions Sweden is imposing.
That's the real Sweden, not the one of covid denial fantasy.
No masks
No business, restaurant or school closures
Sensible advice about how to protect themselves and each other
No new draconian laws implemented inconsistently
No lockdowns
Have I missed something in the link that suggests any of the above are incorrect?
I’m remain confused as the point you are trying to make with this link. Feel free to expand on your argument.
Legal restrictions imposing covid safety measures on bars and restaurants.
https://www.riksdagen.se/sv/dokument-lagar/dokumen...
law said:
SFS No: 2020:526
Ministry/Authority: Ministry of Social
AffairsIssued
: 2020-06-17 Change Register: SFSR (Government Offices)
Source: Full text (Government Offices)
Content:
Transitional provisions
Content and purpose of the law
1 § This law provides for temporary infection control measures to prevent the spread at serving points of the virus causing covid-19.
Definition
2 § For the purposes of this Act, "serving place" means an establishment in which there is an economic activity consisting in serving food or drink to the public and where the possibility of ingestion is permitted on the spot.
Infectious disease control measures
3 § The operator of a serving
area is responsible for 1. the premises of the serving place and the associated outdoor areas to which visitors have access are designed
to avoid congestion and to keep a safe distance from each other from a disease control point of view, 2. activities are organised in such a way as to prevent
the spread of infection among visitors as far as possible, and 3. there are procedures for preventing the spread of infection among visitors.
The first paragraph also applies to entrances to such premises and areas, if the operator of the catering establishment owns or on any other basis disposes of the entrance area.
Supervision
4 § The municipal board responsible for the field of environmental and health protection supervises compliance with this law and related regulations.
The County Administrative Board shall provide support, advice and guidance to the county's municipalities.
5 § At the request of the board referred to in Paragraph 4, the operator of the catering establishment shall provide the information and documents necessary for supervision. The Board has the right to have access to the premises, areas and entrances referred to in Section 3 in order to exercise supervision.
Section 6 On request, the police authority shall provide the board referred to in Section 4 of the Board with the assistance necessary for the application of Section 5.
A request under the first
subparagraph may be made only if 1. it is feared, due to special circumstances, that the measure cannot be taken without the special powers of a police officer under
Section 10 of the Police Act (1984:387) needing to be used, or 2. there are exceptional reasons.
Injunctions and prohibitions
7 § The Board referred to in Section 4 may, in its supervisory activities, order the injunctions and prohibitions necessary for compliance with this law and the connecting regulations.
The Board shall, if necessary, consult the infectious disease control doctor.
Decisions under this Act shall apply immediately unless otherwise specified in the decision.
8 § Decisions pursuant to Paragraph 7(1) may be subject to a penalty payment.
Appeal
9 § Decisions under this Law may be appealed to the general administrative court.
A review permit is required on appeal to the Administrative Court of Appeal.
Authorization
10 § The government or the authority determined by the Government may issue additional provisions on infection control measures in accordance with Section 3.
Transitional provisions
2020:526
1. This Law shall enter into force on 1 July 2020.
2. The Act expires at the end of 2020.
3. However, the repealed law still applies to cases or cases opened before the end of 2020.
The introduced legislation enabling local lockdowns, and are about to start imposing them.Ministry/Authority: Ministry of Social
AffairsIssued
: 2020-06-17 Change Register: SFSR (Government Offices)
Source: Full text (Government Offices)
Content:
Transitional provisions
Content and purpose of the law
1 § This law provides for temporary infection control measures to prevent the spread at serving points of the virus causing covid-19.
Definition
2 § For the purposes of this Act, "serving place" means an establishment in which there is an economic activity consisting in serving food or drink to the public and where the possibility of ingestion is permitted on the spot.
Infectious disease control measures
3 § The operator of a serving
area is responsible for 1. the premises of the serving place and the associated outdoor areas to which visitors have access are designed
to avoid congestion and to keep a safe distance from each other from a disease control point of view, 2. activities are organised in such a way as to prevent
the spread of infection among visitors as far as possible, and 3. there are procedures for preventing the spread of infection among visitors.
The first paragraph also applies to entrances to such premises and areas, if the operator of the catering establishment owns or on any other basis disposes of the entrance area.
Supervision
4 § The municipal board responsible for the field of environmental and health protection supervises compliance with this law and related regulations.
The County Administrative Board shall provide support, advice and guidance to the county's municipalities.
5 § At the request of the board referred to in Paragraph 4, the operator of the catering establishment shall provide the information and documents necessary for supervision. The Board has the right to have access to the premises, areas and entrances referred to in Section 3 in order to exercise supervision.
Section 6 On request, the police authority shall provide the board referred to in Section 4 of the Board with the assistance necessary for the application of Section 5.
A request under the first
subparagraph may be made only if 1. it is feared, due to special circumstances, that the measure cannot be taken without the special powers of a police officer under
Section 10 of the Police Act (1984:387) needing to be used, or 2. there are exceptional reasons.
Injunctions and prohibitions
7 § The Board referred to in Section 4 may, in its supervisory activities, order the injunctions and prohibitions necessary for compliance with this law and the connecting regulations.
The Board shall, if necessary, consult the infectious disease control doctor.
Decisions under this Act shall apply immediately unless otherwise specified in the decision.
8 § Decisions pursuant to Paragraph 7(1) may be subject to a penalty payment.
Appeal
9 § Decisions under this Law may be appealed to the general administrative court.
A review permit is required on appeal to the Administrative Court of Appeal.
Authorization
10 § The government or the authority determined by the Government may issue additional provisions on infection control measures in accordance with Section 3.
Transitional provisions
2020:526
1. This Law shall enter into force on 1 July 2020.
2. The Act expires at the end of 2020.
3. However, the repealed law still applies to cases or cases opened before the end of 2020.
They did ask people to do the same things we asked (or forced) people to do - socially distance, avoid gatherings, wash hands, avoid crowds and public transport, work from home if possible, etc - and people generally complied. Bluntly, I think you and others like you are the reason that wouldn't have worked here. You would have just ignored it.
What I would like to know is what rules were in force in the UK prior to the recent infection surge? Summer seemed largely back to normal for me, although no international travel. What did Sweden do that we didn’t during this time? Or what did Sweden not do that we did? If we excuse their care home deaths, should we not excuse our own?
Sweden are still doing crap compared to many countries. Why would be not look at countries that have largely eradicated the issue? What is it about Sweden?
Sweden are still doing crap compared to many countries. Why would be not look at countries that have largely eradicated the issue? What is it about Sweden?
Killboy said:
What I would like to know is what rules were in force in the UK prior to the recent infection surge? Summer seemed largely back to normal for me, although no international travel. What did Sweden do that we didn’t during this time? Or what did Sweden not do that we did? If we excuse their care home deaths, should we not excuse our own?
Schools were closedgrudas said:
Interesting jump in deaths today
Interesting jump in lockdowns today. Why are hey doing this?https://youtu.be/PRu6Mgb49Uk
Phil. said:
grudas said:
Interesting jump in deaths today
Interesting jump in lockdowns today. Why are hey doing this?https://youtu.be/PRu6Mgb49Uk
otolith said:
Phil. said:
otolith said:
Phil. said:
otolith said:
You keep posting the same link without any explanation expecting others to interpret it for you. Care to explain what point you keep trying to make with this public information link? It lists the measures and restrictions Sweden is imposing.
That's the real Sweden, not the one of covid denial fantasy.
No masks
No business, restaurant or school closures
Sensible advice about how to protect themselves and each other
No new draconian laws implemented inconsistently
No lockdowns
Have I missed something in the link that suggests any of the above are incorrect?
I’m remain confused as the point you are trying to make with this link. Feel free to expand on your argument.
Legal restrictions imposing covid safety measures on bars and restaurants.
https://www.riksdagen.se/sv/dokument-lagar/dokumen...
law said:
SFS No: 2020:526
Ministry/Authority: Ministry of Social
AffairsIssued
: 2020-06-17 Change Register: SFSR (Government Offices)
Source: Full text (Government Offices)
Content:
Transitional provisions
Content and purpose of the law
1 § This law provides for temporary infection control measures to prevent the spread at serving points of the virus causing covid-19.
De?nition
2 § For the purposes of this Act, "serving place" means an establishment in which there is an economic activity consisting in serving food or drink to the public and where the possibility of ingestion is permitted on the spot.
Infectious disease control measures
3 § The operator of a serving
area is responsible for 1. the premises of the serving place and the associated outdoor areas to which visitors have access are designed
to avoid congestion and to keep a safe distance from each other from a disease control point of view, 2. activities are organised in such a way as to prevent
the spread of infection among visitors as far as possible, and 3. there are procedures for preventing the spread of infection among visitors.
The first paragraph also applies to entrances to such premises and areas, if the operator of the catering establishment owns or on any other basis disposes of the entrance area.
Supervision
4 § The municipal board responsible for the field of environmental and health protection supervises compliance with this law and related regulations.
The County Administrative Board shall provide support, advice and guidance to the county's municipalities.
5 § At the request of the board referred to in Paragraph 4, the operator of the catering establishment shall provide the information and documents necessary for supervision. The Board has the right to have access to the premises, areas and entrances referred to in Section 3 in order to exercise supervision.
Section 6 On request, the police authority shall provide the board referred to in Section 4 of the Board with the assistance necessary for the application of Section 5.
A request under the first
subparagraph may be made only if 1. it is feared, due to special circumstances, that the measure cannot be taken without the special powers of a police officer under
Section 10 of the Police Act (1984:387) needing to be used, or 2. there are exceptional reasons.
Injunctions and prohibitions
7 § The Board referred to in Section 4 may, in its supervisory activities, order the injunctions and prohibitions necessary for compliance with this law and the connecting regulations.
The Board shall, if necessary, consult the infectious disease control doctor.
Decisions under this Act shall apply immediately unless otherwise specified in the decision.
8 § Decisions pursuant to Paragraph 7(1) may be subject to a penalty payment.
Appeal
9 § Decisions under this Law may be appealed to the general administrative court.
A review permit is required on appeal to the Administrative Court of Appeal.
Authorization
10 § The government or the authority determined by the Government may issue additional provisions on infection control measures in accordance with Section 3.
Transitional provisions
2020:526
1. This Law shall enter into force on 1 July 2020.
2. The Act expires at the end of 2020.
3. However, the repealed law still applies to cases or cases opened before the end of 2020.
The introduced legislation enabling local lockdowns, and are about to start imposing them.Ministry/Authority: Ministry of Social
AffairsIssued
: 2020-06-17 Change Register: SFSR (Government Offices)
Source: Full text (Government Offices)
Content:
Transitional provisions
Content and purpose of the law
1 § This law provides for temporary infection control measures to prevent the spread at serving points of the virus causing covid-19.
De?nition
2 § For the purposes of this Act, "serving place" means an establishment in which there is an economic activity consisting in serving food or drink to the public and where the possibility of ingestion is permitted on the spot.
Infectious disease control measures
3 § The operator of a serving
area is responsible for 1. the premises of the serving place and the associated outdoor areas to which visitors have access are designed
to avoid congestion and to keep a safe distance from each other from a disease control point of view, 2. activities are organised in such a way as to prevent
the spread of infection among visitors as far as possible, and 3. there are procedures for preventing the spread of infection among visitors.
The first paragraph also applies to entrances to such premises and areas, if the operator of the catering establishment owns or on any other basis disposes of the entrance area.
Supervision
4 § The municipal board responsible for the field of environmental and health protection supervises compliance with this law and related regulations.
The County Administrative Board shall provide support, advice and guidance to the county's municipalities.
5 § At the request of the board referred to in Paragraph 4, the operator of the catering establishment shall provide the information and documents necessary for supervision. The Board has the right to have access to the premises, areas and entrances referred to in Section 3 in order to exercise supervision.
Section 6 On request, the police authority shall provide the board referred to in Section 4 of the Board with the assistance necessary for the application of Section 5.
A request under the first
subparagraph may be made only if 1. it is feared, due to special circumstances, that the measure cannot be taken without the special powers of a police officer under
Section 10 of the Police Act (1984:387) needing to be used, or 2. there are exceptional reasons.
Injunctions and prohibitions
7 § The Board referred to in Section 4 may, in its supervisory activities, order the injunctions and prohibitions necessary for compliance with this law and the connecting regulations.
The Board shall, if necessary, consult the infectious disease control doctor.
Decisions under this Act shall apply immediately unless otherwise specified in the decision.
8 § Decisions pursuant to Paragraph 7(1) may be subject to a penalty payment.
Appeal
9 § Decisions under this Law may be appealed to the general administrative court.
A review permit is required on appeal to the Administrative Court of Appeal.
Authorization
10 § The government or the authority determined by the Government may issue additional provisions on infection control measures in accordance with Section 3.
Transitional provisions
2020:526
1. This Law shall enter into force on 1 July 2020.
2. The Act expires at the end of 2020.
3. However, the repealed law still applies to cases or cases opened before the end of 2020.
They did ask people to do the same things we asked (or forced) people to do - socially distance, avoid gatherings, wash hands, avoid crowds and public transport, work from home if possible, etc - and people generally complied. Bluntly, I think you and others like you are the reason that wouldn't have worked here. You would have just ignored it.
Just what have I done to deserve the statement above? Either tell me or apologise for your deformation of my character! Are you man enough apologise I wonder?
While we’re at it, based on my many years of successful professional leadership and management experience I have discovered that advising and supporting people results in far better behavior than the command and control approach that continues to be levied by this government, particularly when like now there is insufficient scientific justification for their actions (extended lockdowns). That is one of the biggest differences between the Sweden and the UK, and is why Sweden is in a far better place now than the UK.
In case you continue to think lockdowns are effective at stopping COVID then watch this and let’s see if you can continue to tell me why you believe we should be extending lockdowns at the moment across the UK:
https://youtu.be/PRu6Mgb49Uk
Phil. said:
Monkeylegend said:
Classic diversionary tactics there Phil
Have you watched it? Does it resonate? If not what is wrong with the argument presented? Monkeylegend said:
Phil. said:
Monkeylegend said:
Classic diversionary tactics there Phil
Have you watched it? Does it resonate? If not what is wrong with the argument presented? Phil. said:
In case you continue to think lockdowns are effective at stopping COVID then watch this and let’s see if you can continue to tell me why you believe we should be extending lockdowns at the moment across the UK:
https://youtu.be/PRu6Mgb49Uk
Because despite the lack of public events, despite the reduced household mixing, despite the controls already in place, we are seeing (in the case this video of Ireland) real growth in Covid cases week on week in the UK.https://youtu.be/PRu6Mgb49Uk
What we saw back in March last year was a result of large public events still being allowed, hence why we saw the massive numbers of infections. But what we're seeing now is a growth despite the controls that are currently in place, which shows the controls are not being correctly followed.
If we want to return to a time where mass events are possible (and they're not in Sweden), then we need to be in a position where infection rates are incredibly low and the tracking of infection is suitably fast and effective.
Phil. said:
Sweden is in a far better place now than the UK.
There it is again. France (495.57), Moldova (451.23), North Macedonia (406.15), Netherlands (389.3), Ireland (381.58), Iran (375.45), Armenia (369.61), Kosovo (355.5), South Africa (320.04), Romania (304.56), Bosnia and Herzegovina (299.95), Honduras (268.68), Iraq (268.44), Canada (265.31), Israel (254.73), Switzerland (251.04), Costa Rica (240.83), Puerto Rico (240.36), Oman (230.67), Portugal (213.78), Dominican Republic (207.3), Guatemala (205.3), Bahrain (192.43), Kyrgyzstan (175.91), Paraguay (173.52), Kuwait (171.61), Russia (167.53), Albania (158.39), Saudi Arabia (154.33), El Salvador (144.22), Bulgaria (143.5), Czechia (142.39), Ukraine (130.74), Hungary (120.08), Germany (118.68), Denmark¹ (118.33), Turkey (113.84), Serbia (111.43), Libya (109.6), Austria (102.18), Eswatini (102.1), Belarus (98.36), Kazakhstan (96.74), Poland (95.16), Slovenia (91.9), Croatia (91.46), West Bank and Gaza (90.39), India (84.73), Morocco (82.6), Qatar (80.53), Lebanon (76.8), Trinidad and Tobago (69.79), Finland (63.61), Equatorial Guinea (63.41), Azerbaijan (63.37), Philippines (62.59), Egypt (62.28), Tunisia (59.4), Jamaica (58.95), Namibia (53.51), Norway (52.31), Gambia (51.75), Estonia (51.48), Greece (48.47), United Arab Emirates (48.39), Indonesia (47.14), Algeria (44.16), Lithuania (40.51), Afghanistan (40.27), Georgia (38.33), Jordan (38.17), Mauritania (37.02), Australia (36.21), Bangladesh (35.21), Pakistan (31.44), Nepal (26.95), Venezuela (25.49), Gabon (25.48), Nicaragua (23.82), Latvia (22.84), Guinea-Bissau (21.87), Cyprus (21.02), Yemen (20.95), Haiti (20.77), Senegal (20.12), Sudan (20), Zambia (19.94), Lesotho (19.92), Congo (Brazzaville) (17.54), Liberia (17.02), Slovakia (16.89), Cameroon (16.81), Kenya (16.33), Uzbekistan (16.11), Zimbabwe (16.07), Syria (14.85), Uruguay (14.79), Central African Republic (13.29), Japan (13.25), Ethiopia (12.5), Cuba (11.2), Ghana (10.41), Malawi (9.98), Sierra Leone (9.54), Botswana (9.32), Madagascar (9.06), Tajikistan (8.79), South Korea (8.66), Angola (8.05), Mauritius (7.9), Mali (6.92), Somalia (6.6), Togo (6.46), Malaysia (6.03), Chad (6.01), Nigeria (5.74), Guinea (5.64), New Zealand (5.12), South Sudan (5.01), Singapore (4.97), Cote d'Ivoire (4.83), Congo (Kinshasa) (3.6), Benin (3.57), China (3.4), Burkina Faso (3.29), Niger (3.07), Rwanda (2.76), Mozambique (2.54), Uganda (2.27), Thailand (0.85), Papua New Guinea (0.81), Sri Lanka (0.6), Tanzania (0.37), Vietnam (0.37), Burundi (0.09) are all doing better than Sweden with 581.15 deaths per million.
Gassing Station | Speed, Plod & the Law | Top of Page | What's New | My Stuff