CV19 - Cure worse than the disease? (Vol 5)
Discussion


johnboy1975 said:
b0rk said:
anonymous said:
[redacted]
What’s interesting is that none of journals have come out and said why they’re not prepared to publish, is the study flawed in some way? The answer being inconvenient would surely not see publication withheld. After all the now discredited MMR / autism study was first published in the lancet.
Surely the paper and its findings are of scientific interest, and thus everyone in that community wants it publishing and analysing??
Me and my quaint old fashioned common sense view of how the world should work is taking a battering. Not for the first time during this pandemic
Primarily, academic journals are periodicals. There's a limit to how many studies each one can publish. If they have room for 3 studies per issue, and 4 issues a year, and receive 30 studies to publish then they need to be selective.
Each journal has its own set of criteria for publishing. Related content being primary - the journal of avian pathology won't publish a study on bat flu. Secondly, it often can take months, or several years, for a study to be finally published. It can be glacially slow and quite frustrating when a perfectly good study takes forever to worm its way in to print.
In the case of the above study, it is not in the interests of journals to publish multiple studies on the same topic, all at once. The above study is probably not being published due to other similar studies being selected, it has no bearing on the quality of the study. I would, however, expect similar studies with similar results to acknowledge this study and make reference to it.
Bearing in mind that ever since Joseph Lister's germ theory of disease, study after study conclude that the use of surgical masks inhibits the spread of disease, hence why surgeons wear masks during surgery - it is not beyond the realm of possibility that simply dozens of similar studies have been submitted.
wombleh said:
if I was just back off holiday and had to isolate for 14 days and it was keeping me off work then might save on losing 2 weeks income.
Would it though?I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
markyb_lcy said:
Would it though?
I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
Antigen and antibody tests aren’t the same thing?I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
markyb_lcy said:
Would it though?
I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
Yes this is true. If you are told to isolate then its only worth getting a test if you're pretty certain you will test positive.I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
If you test positive you will need to isolate 10 days from symptoms - so this may save you a couple of days in isolation.
If you test negative you still have to isolate for the full 14 days from contact with the infected person so no point in taking the test.
Disastrous said:
stitched said:
In my experience it is not a lack of competence with some parents, just laziness.
A couple I knew who owned the fattest kid in my sons school year were a prime example, the child was invited to a party at my house, 5 kids and I had decided to let them, with supervision, cook cottage pie.
He had never seen potatoes or carrots peeled before. Never seen mince cooked.
12 years of age and never seen a meal cooked. Unable to comprehend that the house contained no crisps, sweets or fizzy drinks.
He actually got embarrassed as he thought I was too poor to supply such things, when I realised what he was thinking I pointed out that the house belonged to me outright, the 2 decent cars were mine and so were the 2 motorcycles in the garage.
That the lack of s te in the cupboards was a lifestyle choice was completely alien to his thinking
te in the cupboards was a lifestyle choice was completely alien to his thinking
I know it's not what you mean but I love the mental picture of an adult angrily setting a child straight on the material value of his assets at a kids party. "No mate, it's an S1000rr and it is NOT on a PCP. This watch? Omega. Your dad got one of them? Didn't think so."A couple I knew who owned the fattest kid in my sons school year were a prime example, the child was invited to a party at my house, 5 kids and I had decided to let them, with supervision, cook cottage pie.
He had never seen potatoes or carrots peeled before. Never seen mince cooked.
12 years of age and never seen a meal cooked. Unable to comprehend that the house contained no crisps, sweets or fizzy drinks.
He actually got embarrassed as he thought I was too poor to supply such things, when I realised what he was thinking I pointed out that the house belonged to me outright, the 2 decent cars were mine and so were the 2 motorcycles in the garage.
That the lack of s
te in the cupboards was a lifestyle choice was completely alien to his thinking

And if you examine THIS bank statement for 2017 you'll see that...
Where's the cringe thread when you need it?

Wiccan of Darkness said:
I ought to comment on this, and reasons why studies aren't published.
Primarily, academic journals are periodicals. There's a limit to how many studies each one can publish. If they have room for 3 studies per issue, and 4 issues a year, and receive 30 studies to publish then they need to be selective.
Each journal has its own set of criteria for publishing. Related content being primary - the journal of avian pathology won't publish a study on bat flu. Secondly, it often can take months, or several years, for a study to be finally published. It can be glacially slow and quite frustrating when a perfectly good study takes forever to worm its way in to print.
In the case of the above study, it is not in the interests of journals to publish multiple studies on the same topic, all at once. The above study is probably not being published due to other similar studies being selected, it has no bearing on the quality of the study. I would, however, expect similar studies with similar results to acknowledge this study and make reference to it.
There are a number of reason why studies don't get published. Space is only one of them. Money and politics could also prevent or delay an inconvenient finding.Primarily, academic journals are periodicals. There's a limit to how many studies each one can publish. If they have room for 3 studies per issue, and 4 issues a year, and receive 30 studies to publish then they need to be selective.
Each journal has its own set of criteria for publishing. Related content being primary - the journal of avian pathology won't publish a study on bat flu. Secondly, it often can take months, or several years, for a study to be finally published. It can be glacially slow and quite frustrating when a perfectly good study takes forever to worm its way in to print.
In the case of the above study, it is not in the interests of journals to publish multiple studies on the same topic, all at once. The above study is probably not being published due to other similar studies being selected, it has no bearing on the quality of the study. I would, however, expect similar studies with similar results to acknowledge this study and make reference to it.
Wiccan of Darkness said:
Bearing in mind that ever since Joseph Lister's germ theory of disease, study after study conclude that the use of surgical masks inhibits the spread of disease, hence why surgeons wear masks during surgery - it is not beyond the realm of possibility that simply dozens of similar studies have been submitted.
The use of surgical masks predates modern medicine's claims to being "evidence based". It is not beyond the realms of possibility that it is a retained superstition. Certainly it isn't proven -https://pubmed.ncbi.nlm.nih.gov/1853618/
djc206 said:
markyb_lcy said:
Would it though?
I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
Antigen and antibody tests aren’t the same thing?I have a friend who ended up with a negative (antigen) test after being identified as being in close contact with someone who tested positive.
Test and trace still advised and expected him to isolate regardless of the negative result. Not doing so could result in a fine.
Certainly an antibody test cant/ shouldn’t be used as a measure as to whether to isolate or not because not everybody develops antibodies and you’re likely to be infectious before you do.
Antibody test tells you if your body has current antibodies which may provide immunity from infection.
markyb_lcy said:
Antigen test tells you if you have an active infection (false positive and detection of dead fragments problems aside).
Antibody test tells you if your body has current antibodies which may provide immunity from infection.
Yep. Sorry I think I must have confused your point in the other post. Ignore me!Antibody test tells you if your body has current antibodies which may provide immunity from infection.
Daily cases by specimen date are varying significantly, between 14k and 25K in the last week.
Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
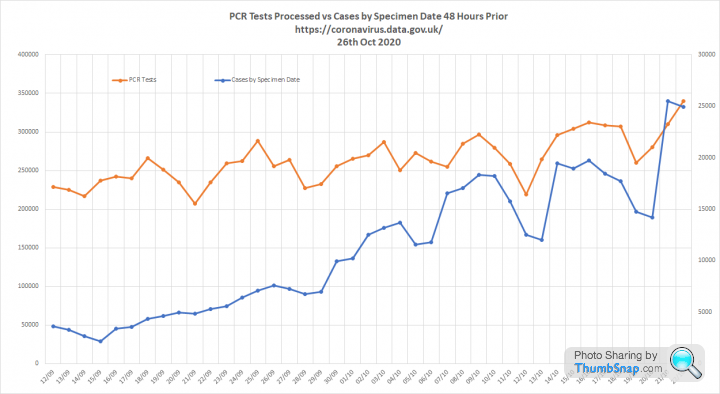
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
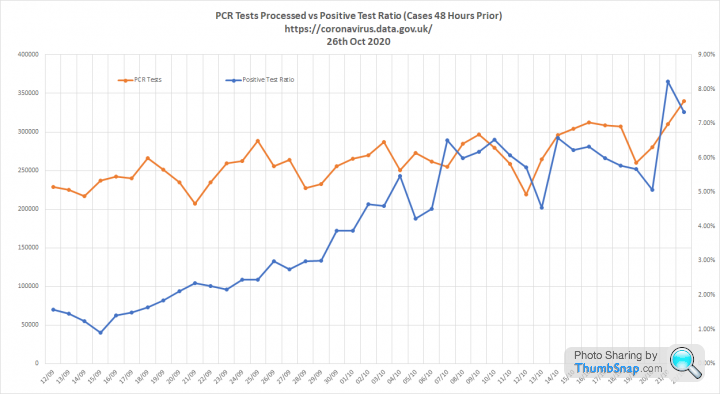
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
johnboy1975 said:
Darth Paul said:
CrutyRammers said:
Elysium said:
That really puts this in perspective doesn't it?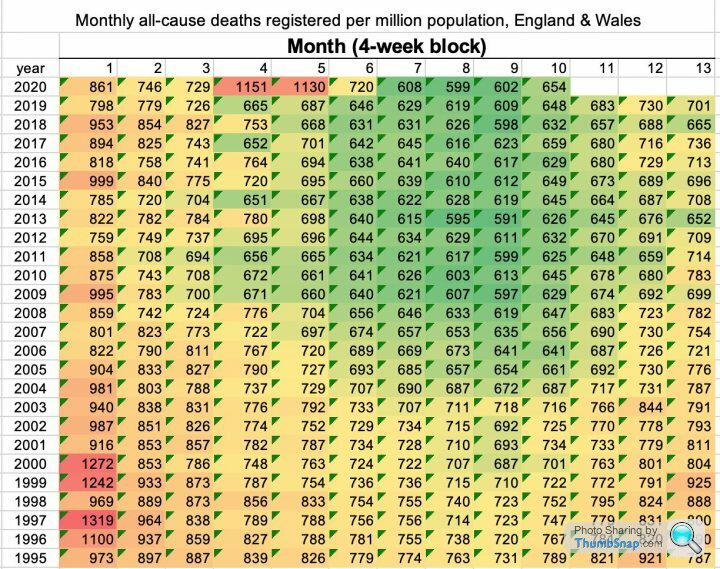
Edit to add that is about a 6% increase on last September which looked a very average number for a September. And to also add I’m playing a bit of devils advocate on this as I’m very much on the Yeadon end of the playground for this one.
Edited by Darth Paul on Monday 26th October 10:25
Lots of green on that graph in recent times, seems we've been storing up problems for quite a while.....2004 and before are noticeably worse. Overall 2020 looks fairly unremarkable
I heard 2020 was the 8th worst for deaths in recent times, that heatmap would appear to back that up. Tellingly, we didnt do all this s
t the other 7 timesElysium said:
Daily cases by specimen date are varying significantly, between 14k and 25K in the last week.
Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
You're right in that you wouldn't expect that to happen. But I'd want to see a couple of week's more correlation before I was convinced there's anything there; at the moment I'd file that under "something to keep an eye on" rather than definitive proof. It is certainly worth watching as it does seem rather odd.Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
CrutyRammers said:
Elysium said:
Daily cases by specimen date are varying significantly, between 14k and 25K in the last week.
Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
You're right in that you wouldn't expect that to happen. But I'd want to see a couple of week's more correlation before I was convinced there's anything there; at the moment I'd file that under "something to keep an eye on" rather than definitive proof. It is certainly worth watching as it does seem rather odd.Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
The false positives thing really needs following up though, especially as we head towards 500k a day (within the week?)
Has the idea that the test can return positive if other coronaviruses are present been debunked yet? Its shocking if true, I cant quite believe they would be so stupid. Plus the positivity rate would probably be higher?
CrutyRammers said:
Elysium said:
Daily cases by specimen date are varying significantly, between 14k and 25K in the last week.
Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
You're right in that you wouldn't expect that to happen. But I'd want to see a couple of week's more correlation before I was convinced there's anything there; at the moment I'd file that under "something to keep an eye on" rather than definitive proof. It is certainly worth watching as it does seem rather odd.Daily PCR swabs processed is also varying considerably between 260k and 340k over a similar period.
I wanted to understand how these variances might interact, so I put together this graph, which compares test numbers with cases by specimen date 2 days prior:
In september, day to day changes in the number of tests did not make a big difference to the number of cases. However, this has changed during October and there is now a close correlation.
My first thought was that the availability of tests is a limiting factor. So the more we test the more cases we find. If this is true the %'age of positive tests should be similar day to day. However it isn't:
The %'age of positive test results is increasing as numbers of tests increase and falling as they reduce. This should not be happening. It should either fall or remain constant.
I think this is evidence of a significant problem with the testing process as Mike Yeadon has suggested.
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
A: more people actually have the virus.
B: testing has been targeted to find these people (on campus testing for students etc)
Bullett said:
Elysium said:
Stuff....
More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
Could it not also indicate more focused testing? You should only be tested if you have symptoms, is that message getting through. More tests leading to a greater percentage of positive results could indicate an increase in the error rate in the laboratories.
I can't think of a mechanism that would cause that.
johnboy1975 said:
Isn't the percentage of positive cases just a function of how many asymptomatic people they rounded up on a particular day? Like you both, I would have thought more tests = lower positive %, but its pretty random, ie on a given day you could have a lot of people with symptoms getting tested or a greater amount of positive asymptomatic tests.
The false positives thing really needs following up though, especially as we head towards 500k a day (within the week?)
Has the idea that the test can return positive if other coronaviruses are present been debunked yet? Its shocking if true, I cant quite believe they would be so stupid. Plus the positivity rate would probably be higher?
I think that the PCR test cycle threshold is going to be the much bigger issue. The false positives thing really needs following up though, especially as we head towards 500k a day (within the week?)
Has the idea that the test can return positive if other coronaviruses are present been debunked yet? Its shocking if true, I cant quite believe they would be so stupid. Plus the positivity rate would probably be higher?
To my mind this is a bit like the anomaly that CEBM identified on the way we were recording deaths. In the beginning, it makes sense that any death of a person testing positive should be counted. At that point the only positive tests were of very sick people in hospital.
Fast forward a couple of months through large scale testing and the knowledge that at least 5 million people have had the virus and it makes no sense at all. Limiting COVID deaths to those within 28 days of a positive test is much better, but still bluntly innacurate.
The cycle count issue is similar. At the start, anyone with symptoms and any quantity of the virus in their bodies is a case. Later on, with 5 million people infected you have a big group with some traces of this stuff who are no longer ill. Ramp up your testing over a 2 month period as we have now done and you will always find more 'cases'.
60% of all cases have been found in the 50 or so days since the August bank holiday. Half of all of the testing has been done in the same period.
13 million tests!
Elysium said:
More focused testing and greater prevalence should increase the positivity rate, but I am not sure that explains why it would increase and decrease day to day in line with the number of tests.
I can't think of a mechanism that would cause that.
It could if there are instances of day-long focussed testing (e.g. a testing station is opened at a university and all the poorly kids get tested on the first day). I think seeing a random walk is not very surprising in itself. The scale of variation from day to day is slightly surprising. I can't think of a mechanism that would cause that.
Elysium said:
johnboy1975 said:
Isn't the percentage of positive cases just a function of how many asymptomatic people they rounded up on a particular day? Like you both, I would have thought more tests = lower positive %, but its pretty random, ie on a given day you could have a lot of people with symptoms getting tested or a greater amount of positive asymptomatic tests.
The false positives thing really needs following up though, especially as we head towards 500k a day (within the week?)
Has the idea that the test can return positive if other coronaviruses are present been debunked yet? Its shocking if true, I cant quite believe they would be so stupid. Plus the positivity rate would probably be higher?
I think that the PCR test cycle threshold is going to be the much bigger issue. The false positives thing really needs following up though, especially as we head towards 500k a day (within the week?)
Has the idea that the test can return positive if other coronaviruses are present been debunked yet? Its shocking if true, I cant quite believe they would be so stupid. Plus the positivity rate would probably be higher?
To my mind this is a bit like the anomaly that CEBM identified on the way we were recording deaths. In the beginning, it makes sense that any death of a person testing positive should be counted. At that point the only positive tests were of very sick people in hospital.
Fast forward a couple of months through large scale testing and the knowledge that at least 5 million people have had the virus and it makes no sense at all. Limiting COVID deaths to those within 28 days of a positive test is much better, but still bluntly innacurate.
The cycle count issue is similar. At the start, anyone with symptoms and any quantity of the virus in their bodies is a case. Later on, with 5 million people infected you have a big group with some traces of this stuff who are no longer ill. Ramp up your testing over a 2 month period as we have now done and you will always find more 'cases'.
60% of all cases have been found in the 50 or so days since the August bank holiday. Half of all of the testing has been done in the same period.
13 million tests!
https://www.spectator.co.uk/article/why-did-the-fl...
You'd have to consider if similar was happening here. But surely, given only 5 people have had Covid-19 twice, people would be going to the press (in ever increasing numbers) with tales of double infection?
ORD said:
Elysium said:
More focused testing and greater prevalence should increase the positivity rate, but I am not sure that explains why it would increase and decrease day to day in line with the number of tests.
I can't think of a mechanism that would cause that.
It could if there are instances of day-long focussed testing (e.g. a testing station is opened at a university and all the poorly kids get tested on the first day). I think seeing a random walk is not very surprising in itself. The scale of variation from day to day is slightly surprising. I can't think of a mechanism that would cause that.
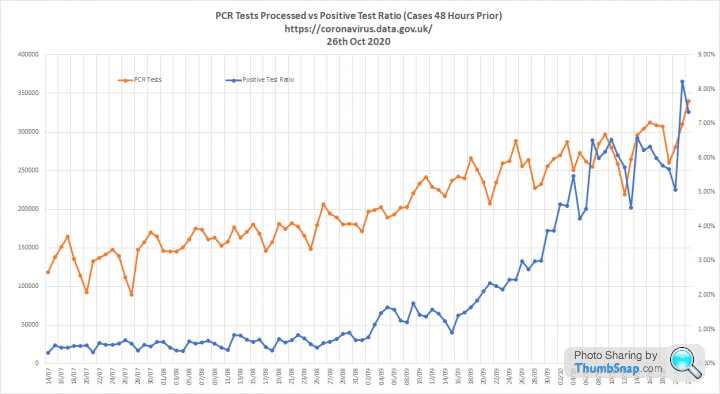
It's less obvious, but you can see dips in the positive test rate when testing volumes fell back in July.
More tests seems to lead to a higher %'age positive, which is counterintuitive.
Elysium said:
ORD said:
Elysium said:
More focused testing and greater prevalence should increase the positivity rate, but I am not sure that explains why it would increase and decrease day to day in line with the number of tests.
I can't think of a mechanism that would cause that.
It could if there are instances of day-long focussed testing (e.g. a testing station is opened at a university and all the poorly kids get tested on the first day). I think seeing a random walk is not very surprising in itself. The scale of variation from day to day is slightly surprising. I can't think of a mechanism that would cause that.
It's less obvious, but you can see dips in the positive test rate when testing volumes fell back in July.
More tests seems to lead to a higher %'age positive, which is counterintuitive.
Which could be:
Genuine rising of infections
And/or
Old fragment positivity increasing
Would 7 day averages smooth it out a bit?
EDIT
If you are still using the "2 days prior" that might be an issue, in that earlier on, tests were processed same day or next day. Just a thought
Edited by johnboy1975 on Monday 26th October 14:52
Gassing Station | News, Politics & Economics | Top of Page | What's New | My Stuff