Coronavirus - Data Analysis Thread
Discussion


CarlosFandango11 said:
Ashfordian said:
havoc said:
Their age-groupings are ridiculous:-
- 0-5
- 6-17
- 18-54 (!!!)
- 55-64
- 65-74
- 75-84
- 85+
- Unknown
I can, to a degree, understand the greater graduations at the bottom and top end of the scale, but lumping 36 years of adults together is an utter joke...how the hell can our civil service not do statistics decently???
I believe the 18-54 age grouping is intentional. Splitting it up would simply demonstrate the younger are at miniscule risk and out the scaremongering they have been doing for the last 15 months for a large section of the adult population.- 0-5
- 6-17
- 18-54 (!!!)
- 55-64
- 65-74
- 75-84
- 85+
- Unknown
I can, to a degree, understand the greater graduations at the bottom and top end of the scale, but lumping 36 years of adults together is an utter joke...how the hell can our civil service not do statistics decently???
What I'm after (and not going to get) is the data that would show whether we're seeing a shrunk copy of the old stratification (where the older you are the greater the risk is, albeit with all vaccinated groups shifted significantly downwards) or whether the data is broadly 'flat' across all age groups, which would (IMHO) suggest that only those with specific risk factors (asthma, diabetes, obesity...) are being hospitalised.
...and yes, I do have personal interest in this, especially after Boris telling us all to "live* with it" this evening!
* That could be a very unfortunate choice of words for +/- 15 people a day...or more if things keep ramping up as they appear very likely to...
CarlosFandango11 said:
Ashfordian said:
havoc said:
Their age-groupings are ridiculous:-
- 0-5
- 6-17
- 18-54 (!!!)
- 55-64
- 65-74
- 75-84
- 85+
- Unknown
I can, to a degree, understand the greater graduations at the bottom and top end of the scale, but lumping 36 years of adults together is an utter joke...how the hell can our civil service not do statistics decently???
I believe the 18-54 age grouping is intentional. Splitting it up would simply demonstrate the younger are at miniscule risk and out the scaremongering they have been doing for the last 15 months for a large section of the adult population.- 0-5
- 6-17
- 18-54 (!!!)
- 55-64
- 65-74
- 75-84
- 85+
- Unknown
I can, to a degree, understand the greater graduations at the bottom and top end of the scale, but lumping 36 years of adults together is an utter joke...how the hell can our civil service not do statistics decently???
We have known since the start that issues with Covid is massively skewed to older people.
havoc said:
Jinx said:
Looks good but it does worry me slightly that we are in the middle of summer and are doing 4x as many tests as we were doing back in Autumn last year. If we normalise for the number of tests (whilst assuming the underlying infection rates in the general population are similar) then the number of hospitalisations isn't so optimistic. i.e. last September we had a similar hospitalisation rate with around half to a third the number of positive tests - but the number of tests was a quarter of what we are doing now.
I'm not sure you can compare that directly...different circumstances Last Autumn we were only recently out of a lockdown, people were being ultra-cautious, and there were almost no "events" happening. Plus pubs weren't allowing people inside, employers weren't pushing people back into offices, etc. etc. So risky behaviours and opportunities for infection were both much lower 9 months ago.
Compare to now, and we've got massive spectator-filled events happening, pubs full of drunken people hugging each other, and at least half the population suffering from pandemic ennui and wanting/wishing the whole thing over...driving arguably more risky/inappropriate behaviours. Add in a government which has jumped the shark as far as credibility goes, and is busy sending out messages that everything is going to be OK, and it's not surprising things are going the wrong way.
The big issue for me is (as you allude to) that hospitalisation line, and how that links to the death rate (is the trend improving or worsening) - if the hospitalisation line manages to stay pretty flat despite the rampant cases, then the desire to re-open will seem perfectly reasonable. If it climbs noticeably in coming weeks, and doubly so if it brings the death #s up with it, then there's an argument to say that we should take (have taken) an intermediate step before full release.
(Would also be nice to see a "Long Covid" rate, but almost no-one seems to care about that.)

As for long covid, afaik this is people self certifying that they have problems not a jot of science to it + they may well be unwell people anyway before covid and/or chancers.
TX.
havoc said:
I'm not sure you can compare that directly...different circumstances
Last Autumn we were only recently out of a lockdown, people were being ultra-cautious, and there were almost no "events" happening. Plus pubs weren't allowing people inside, employers weren't pushing people back into offices, etc. etc. So risky behaviours and opportunities for infection were both much lower 9 months ago.
Compare to now, and we've got massive spectator-filled events happening, pubs full of drunken people hugging each other, and at least half the population suffering from pandemic ennui and wanting/wishing the whole thing over...driving arguably more risky/inappropriate behaviours. Add in a government which has jumped the shark as far as credibility goes, and is busy sending out messages that everything is going to be OK, and it's not surprising things are going the wrong way.
The big issue for me is (as you allude to) that hospitalisation line, and how that links to the death rate (is the trend improving or worsening) - if the hospitalisation line manages to stay pretty flat despite the rampant cases, then the desire to re-open will seem perfectly reasonable. If it climbs noticeably in coming weeks, and doubly so if it brings the death #s up with it, then there's an argument to say that we should take (have taken) an intermediate step before full release.
(Would also be nice to see a "Long Covid" rate, but almost no-one seems to care about that.)
https://www.instituteforgovernment.org.uk/sites/de... Mid August restrictions were lifted and at the tail end of September (just after the eat out to help out) the Rule of 6 was brought in with the working from home edict (so pretty much what we have now) and it wasn't until October that the tier system was brought in. So the period August to September was as open as things will be in 2 weeks time (though with masks).Last Autumn we were only recently out of a lockdown, people were being ultra-cautious, and there were almost no "events" happening. Plus pubs weren't allowing people inside, employers weren't pushing people back into offices, etc. etc. So risky behaviours and opportunities for infection were both much lower 9 months ago.
Compare to now, and we've got massive spectator-filled events happening, pubs full of drunken people hugging each other, and at least half the population suffering from pandemic ennui and wanting/wishing the whole thing over...driving arguably more risky/inappropriate behaviours. Add in a government which has jumped the shark as far as credibility goes, and is busy sending out messages that everything is going to be OK, and it's not surprising things are going the wrong way.
The big issue for me is (as you allude to) that hospitalisation line, and how that links to the death rate (is the trend improving or worsening) - if the hospitalisation line manages to stay pretty flat despite the rampant cases, then the desire to re-open will seem perfectly reasonable. If it climbs noticeably in coming weeks, and doubly so if it brings the death #s up with it, then there's an argument to say that we should take (have taken) an intermediate step before full release.
(Would also be nice to see a "Long Covid" rate, but almost no-one seems to care about that.)
It is the best period to compare with as we have better data from that period (than the first "peak") and it wasn't during the winter months.
Long Covid is difficult to quantify as there isn't a test for it and separating long covid from the long term effects of intubation is again difficult to do. At the moment I would say the jury is out but then I don't have access to the full hospitalisation data.
Ashfordian said:
CarlosFandango11 said:
Ashfordian said:
havoc said:
Their age-groupings are ridiculous:-
- 0-5
- 6-17
- 18-54 (!!!)
- 55-64
- 65-74
- 75-84
- 85+
- Unknown
I can, to a degree, understand the greater graduations at the bottom and top end of the scale, but lumping 36 years of adults together is an utter joke...how the hell can our civil service not do statistics decently???
I believe the 18-54 age grouping is intentional. Splitting it up would simply demonstrate the younger are at miniscule risk and out the scaremongering they have been doing for the last 15 months for a large section of the adult population.- 0-5
- 6-17
- 18-54 (!!!)
- 55-64
- 65-74
- 75-84
- 85+
- Unknown
I can, to a degree, understand the greater graduations at the bottom and top end of the scale, but lumping 36 years of adults together is an utter joke...how the hell can our civil service not do statistics decently???
We have known since the start that issues with Covid is massively skewed to older people.
If you want to see the risk of Covid to various age ranges, then there's plenty of death & case data split by 5 year age ranges available. This 18-54 age group has clearly not been chosen to hide anything like you're implying.
Update on todays data
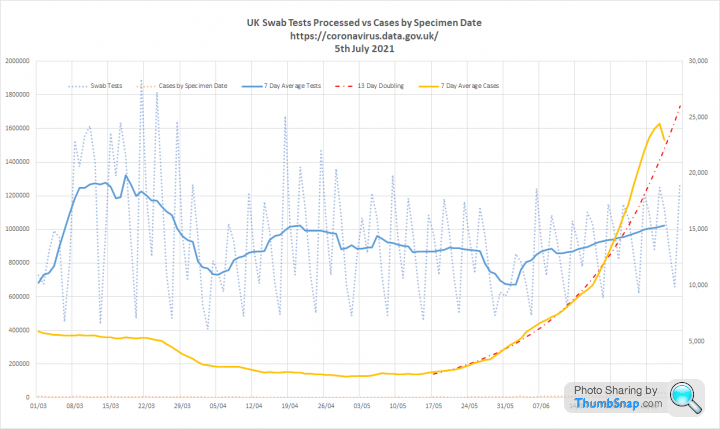
1. Tests are slowing increasing. Back at April levels with a 7 day average of over 1m per day. Cases had accelerated away from the earlier 13 day doubling, but growth seems to be slowing. The apparent peak on the graph is reporting lag over the last couple of days:
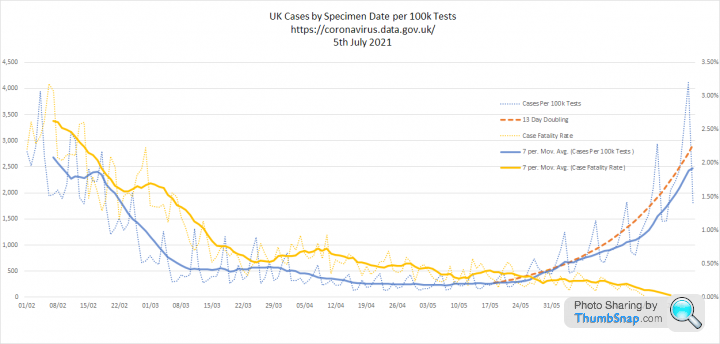
Slightly different picture when you correct for testing. But the main thing to note here is the steadily falling 'case fatality rate'. The 7 day average, which relates to cases up to 21st June is now 1 in 1,000:
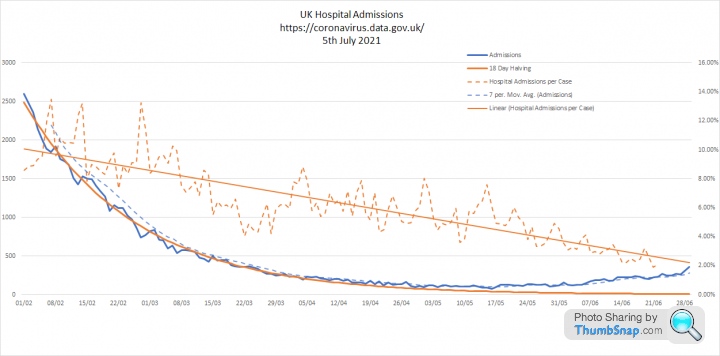
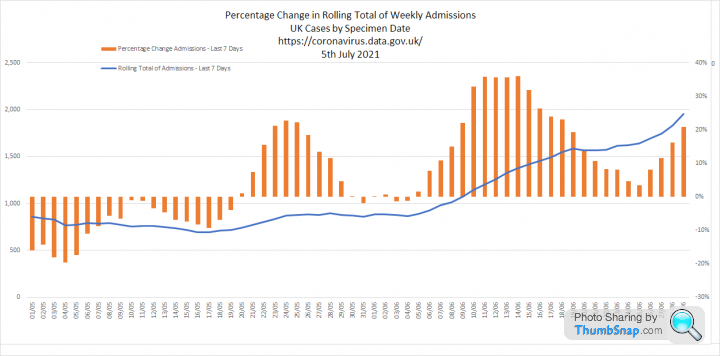
2. A similar picture with admissions. Although they are increasing in absolute terms, the percentage of cases resulting in admission to hospital is steadily decreasing. 7 day average of 2.5% for cases up to the 21st June. 25 per 1000 people.
3. This shows cases per 100k tests, admissions and deaths overlaid with an appropriate lag. Although this is still looking good we are getting to the point where the acceleration in cases might begin to be seen in admissions and deaths. We need to watch over the next 2 weeks and hold our nerve:

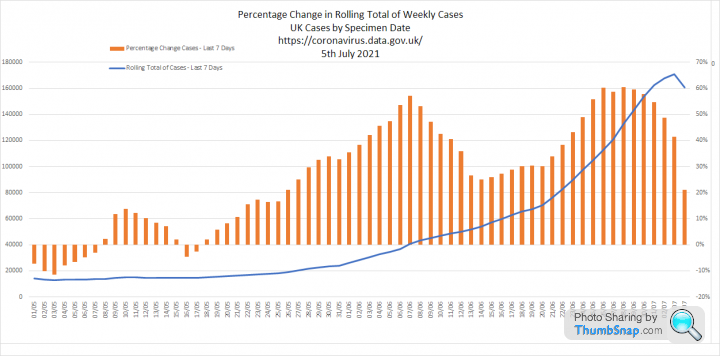
4. These last two graphs look at the growth rate for cases and admissions. Case growth is slowing and there is some hope we might hit a peak soon. The Universities breaking up for the summer could help here. As will the school holidays when mass LFD testing is likely to slow down. Admissions are still growing, but they lag cases by a week:
All in all, I think we are in good shape to keep going and ride out the exit wave.
1. Tests are slowing increasing. Back at April levels with a 7 day average of over 1m per day. Cases had accelerated away from the earlier 13 day doubling, but growth seems to be slowing. The apparent peak on the graph is reporting lag over the last couple of days:
Slightly different picture when you correct for testing. But the main thing to note here is the steadily falling 'case fatality rate'. The 7 day average, which relates to cases up to 21st June is now 1 in 1,000:
2. A similar picture with admissions. Although they are increasing in absolute terms, the percentage of cases resulting in admission to hospital is steadily decreasing. 7 day average of 2.5% for cases up to the 21st June. 25 per 1000 people.
3. This shows cases per 100k tests, admissions and deaths overlaid with an appropriate lag. Although this is still looking good we are getting to the point where the acceleration in cases might begin to be seen in admissions and deaths. We need to watch over the next 2 weeks and hold our nerve:
4. These last two graphs look at the growth rate for cases and admissions. Case growth is slowing and there is some hope we might hit a peak soon. The Universities breaking up for the summer could help here. As will the school holidays when mass LFD testing is likely to slow down. Admissions are still growing, but they lag cases by a week:
All in all, I think we are in good shape to keep going and ride out the exit wave.
Terminator X said:
It isn't "going the wrong way" though, deaths almost non existent as are hospitalizations. Why we are even reporting daily covid deaths is driving me
The hospitalisation curve, as per Elysium's data above, IS going the wrong way, despite an ever-increasing number of people vaccinated. Over half of those people HAVE been vaccinated, just to be clear. I would also suggest the majority of those still dying HAVE been vaccinated. ...and Boris has just told all the "couldn't give a s
 t'ers" like you to go do what you like...which WILL increase the spread of the damn thing.
t'ers" like you to go do what you like...which WILL increase the spread of the damn thing.As for the death rate, it's currently comparable to suicides per year and it's >2x as deadly as driving (on average) in the UK.
...of which the latter has the benefit of being an activity where you can manage your own risk. So I agree it's not significant, and I understand (and agree with!) the economic rationale for allowing more places to open, more events to happen.
But where's the logic in ditching mask-wearing, in ditching social-distancing? In effectively telling everyone it's over??? (Which, let's be honest, is the message the great unwashed WILL take away...)
I will wager both hospitalisations and deaths will increase across the summer as restrictions are lifted and people go on holiday across the UK. Where it goes in Sept/Oct is an interesting question, but the virus will* again increase in prevalence in Nov/Dec/Jan/Feb as all coronaviruses do across the colder months. So the current +/- 15 a day is likely to be a low point for much of the rest of the year. (although whether it only goes to ~20 or up past 50/day is entirely unknown...)
Terminator X said:
As for long covid, afaik this is people self certifying that they have problems not a jot of science to it + they may well be unwell people anyway before covid and/or chancers.
Right... 
...so professional people with careers they care about and the self-employed are "chancers"?!? And I suppose you think ME isn't real, either? And that stress and depression are self-inflicted and those people need to pull themselves together???
* Pending any more mutations which may change its characteristics
PS - Elysium - given the massive # of tests now being performed vs last year, I suggest the "x per 100,000 tests" measure is no longer reliable...certainly it's not comparable with historic data.
havoc said:
PS - Elysium - given the massive # of tests now being performed vs last year, I suggest the "x per 100,000 tests" measure is no longer reliable...certainly it's not comparable with historic data.
That’s why we should correct for testing. Cases now cannot be compared with cases a year ago. Our explosion in testing only began last Autumn. Elysium said:
That’s why we should correct for testing. Cases now cannot be compared with cases a year ago. Our explosion in testing only began last Autumn.
Yes...ish.Cases...yes, I can see the argument. Although historically most tests were in hospital/care-home environments - where prevalence was higher than average. So I'd expect to see a drop in the rate anyway once testing was expanded to general population, especially when there's a lot of random tests e.g. at work.
...so correction for testing is definitely better than doing nothing, but hides expected statistical deviations.
Hospitalisations - not relevant. That's an absolute figure.
Deaths - ditto.
havoc said:
Elysium said:
That’s why we should correct for testing. Cases now cannot be compared with cases a year ago. Our explosion in testing only began last Autumn.
Yes...ish.Cases...yes, I can see the argument. Although historically most tests were in hospital/care-home environments - where prevalence was higher than average. So I'd expect to see a drop in the rate anyway once testing was expanded to general population, especially when there's a lot of random tests e.g. at work.
...so correction for testing is definitely better than doing nothing, but hides expected statistical deviations.
Hospitalisations - not relevant. That's an absolute figure.
Deaths - ditto.
I am using absolute figures for hospitalisation and deaths, although it should be understood that they also ultimately relate to testing levels.
Hospitalisation rates are also a function of human behaviour and NHS capacity. It makes sense that we would admit more mild cases when the NHS has capacity and limit it to severe cases when it does not.
.
Jinx said:
This is a really useful graphic of the timeline, thanks for posting the link 
havoc said:
Elysium said:
That’s why we should correct for testing. Cases now cannot be compared with cases a year ago. Our explosion in testing only began last Autumn.
Yes...ish.Cases...yes, I can see the argument. Although historically most tests were in hospital/care-home environments - where prevalence was higher than average. So I'd expect to see a drop in the rate anyway once testing was expanded to general population, especially when there's a lot of random tests e.g. at work.
...so correction for testing is definitely better than doing nothing, but hides expected statistical deviations.
Hospitalisations - not relevant. That's an absolute figure.
Deaths - ditto.
there were 103 admissions on 29th May and 358 on 29th June.
On the same date there were 884 people in hospital in May and 1726 in June
So while admissions increased by 3.5 times those in hospital only doubled.
Is it really relevant for decision making how many people in hospital have tested positive for covid? Presumably when there’s more cases in the community, there will be more in the hospitals whether or not they are there because of coronavirus.
I’m only really paying attention to the ICU numbers.
I’m only really paying attention to the ICU numbers.
simoid said:
Is it really relevant for decision making how many people in hospital have tested positive for covid? Presumably when there’s more cases in the community, there will be more in the hospitals whether or not they are there because of coronavirus.
I’m only really paying attention to the ICU numbers.
Yes, it gives an idea of how effective the level of vaccination is, and whether it's likely the hospitals will reach capacity in the near future.I’m only really paying attention to the ICU numbers.
I just dont get the current relaxing of rules. Around the 19th we are probably going to be approaching the peak of the current wave. I can only guess the are stress testing the vaccine.
I would rather have another 4 weeks of the rules we are currently under to get another 20% or so of 2nd doses and then lift the restrictions as the cases will be falling by then anyway. (hopefully)
Only time will tell after the 19th but I dont think this will end well. Its all well and good saying but hospital admissions are low but when you have businesses crippled with people off with covid its just as bad. I know of several local businesses that have had to close in the last few weeks as they just dont have the staff due to people +ve with covid.
My industry is really starting to feel it now in the supply chain.
I would rather have another 4 weeks of the rules we are currently under to get another 20% or so of 2nd doses and then lift the restrictions as the cases will be falling by then anyway. (hopefully)
Only time will tell after the 19th but I dont think this will end well. Its all well and good saying but hospital admissions are low but when you have businesses crippled with people off with covid its just as bad. I know of several local businesses that have had to close in the last few weeks as they just dont have the staff due to people +ve with covid.
My industry is really starting to feel it now in the supply chain.
red_slr said:
I just dont get the current relaxing of rules. Around the 19th we are probably going to be approaching the peak of the current wave. I can only guess the are stress testing the vaccine.
I would rather have another 4 weeks of the rules we are currently under to get another 20% or so of 2nd doses and then lift the restrictions as the cases will be falling by then anyway. (hopefully)
Only time will tell after the 19th but I dont think this will end well. Its all well and good saying but hospital admissions are low but when you have businesses crippled with people off with covid its just as bad. I know of several local businesses that have had to close in the last few weeks as they just dont have the staff due to people +ve with covid.
My industry is really starting to feel it now in the supply chain.
Think of the R number as an accelerator on a machine that makes widgets. I would rather have another 4 weeks of the rules we are currently under to get another 20% or so of 2nd doses and then lift the restrictions as the cases will be falling by then anyway. (hopefully)
Only time will tell after the 19th but I dont think this will end well. Its all well and good saying but hospital admissions are low but when you have businesses crippled with people off with covid its just as bad. I know of several local businesses that have had to close in the last few weeks as they just dont have the staff due to people +ve with covid.
My industry is really starting to feel it now in the supply chain.
At R of 1.4 we have constant acceleration. Every 5 days the machine speeds up 40%. It will contine to accelerate and we will continue to stack up widgets until it eventually runs out of fuel.
Thats where we are now. Its an exit wave and its going to continue until we have sufficient levels of immunity to slow the spread. The issue is that vaccine derived immunity is not total. Although 86% of adults have had a first dose of the vaccine, this 'wall' of immunity is permeable. The good news is that the breakthrough infections are clearly increasingly mild.
So what are our options:
1. Try to stop it
That would mean going back into lockdown. But we don't actually know if our original lockdown measures would be enough to reverse the growth of the new variant.
More significantly since people are no longer dying of COVID in any significant numbers its difficult to see a lawful justification for this option.
2. Slow it down / stay as we are
We really need the exit wave to peak before the Autumn. The less it overlaps with usual winter pressures on the NHS the better. Slowing it down could drive the peak into winter, which will be really really unhelpful
3. Continue to unlock
This actually ends up being the only option. The summer is the best time for the exit wave to occur because its when the NHS has the most flex to deal with it.
Elysium said:
Think of the R number as an accelerator on a machine that makes widgets.
At R of 1.4 we have constant acceleration. Every 5 days the machine speeds up 40%. It will contine to accelerate and we will continue to stack up widgets until it eventually runs out of fuel.
Thats where we are now. Its an exit wave and its going to continue until we have sufficient levels of immunity to slow the spread. The issue is that vaccine derived immunity is not total. Although 86% of adults have had a first dose of the vaccine, this 'wall' of immunity is permeable. The good news is that the breakthrough infections are clearly increasingly mild.
So what are our options:
1. Try to stop it
That would mean going back into lockdown. But we don't actually know if our original lockdown measures would be enough to reverse the growth of the new variant.
More significantly since people are no longer dying of COVID in any significant numbers its difficult to see a lawful justification for this option.
2. Slow it down / stay as we are
We really need the exit wave to peak before the Autumn. The less it overlaps with usual winter pressures on the NHS the better. Slowing it down could drive the peak into winter, which will be really really unhelpful
3. Continue to unlock
This actually ends up being the only option. The summer is the best time for the exit wave to occur because its when the NHS has the most flex to deal with it.
It is definitely a case of now or never - at the moment the NHS can cope with a projected number of cases over the summer with opening up. This will not be the case any later in the year. At R of 1.4 we have constant acceleration. Every 5 days the machine speeds up 40%. It will contine to accelerate and we will continue to stack up widgets until it eventually runs out of fuel.
Thats where we are now. Its an exit wave and its going to continue until we have sufficient levels of immunity to slow the spread. The issue is that vaccine derived immunity is not total. Although 86% of adults have had a first dose of the vaccine, this 'wall' of immunity is permeable. The good news is that the breakthrough infections are clearly increasingly mild.
So what are our options:
1. Try to stop it
That would mean going back into lockdown. But we don't actually know if our original lockdown measures would be enough to reverse the growth of the new variant.
More significantly since people are no longer dying of COVID in any significant numbers its difficult to see a lawful justification for this option.
2. Slow it down / stay as we are
We really need the exit wave to peak before the Autumn. The less it overlaps with usual winter pressures on the NHS the better. Slowing it down could drive the peak into winter, which will be really really unhelpful
3. Continue to unlock
This actually ends up being the only option. The summer is the best time for the exit wave to occur because its when the NHS has the most flex to deal with it.
Can I just say - bloody second jab - had it yesterday and now I ache all over including my eyes...
Vanden Saab said:
hospitalizations are not absolute. Only the number in hospital is. If 300 people a day are hospitalized but 350 are leaving hospital for example.
there were 103 admissions on 29th May and 358 on 29th June.
On the same date there were 884 people in hospital in May and 1726 in June
So while admissions increased by 3.5 times those in hospital only doubled.
You're right, but you've missed my point - if we're talking about the # of people requiring hospitalisation following contagion, then it's admissions which matter, and that figure is the same regardless of testing.there were 103 admissions on 29th May and 358 on 29th June.
On the same date there were 884 people in hospital in May and 1726 in June
So while admissions increased by 3.5 times those in hospital only doubled.
Elysium - good points about the capacity of hospitals / ability to admit more minor cases now / ITU being a focus.
Terminator X said:
It seems this will never end for you which is a shame. All the best with it.
You really are an arrogant, patronising tt, aren't you?!?Elysium said:
Think of the R number as an accelerator on a machine that makes widgets.
...
So what are our options:
1. Try to stop it
2. Slow it down / stay as we are
3. Continue to unlock
Interesting perspective...and statistically persuasive....
So what are our options:
1. Try to stop it
2. Slow it down / stay as we are
3. Continue to unlock
I would throw a few challenges at that though:-
1) We're dealing with individuals, who aren't (at all) logical, on both sides. So you'll have those deliberately getting in other people's faces because they can, and at the other end of the scale it will lead to those individuals feeling vulnerable or suffering from anxiety being effectively pushed back into isolating in their homes (which will exacerbate any pre-existing mental health issues) because they can no longer rely on their fellow countrymen behaving reasonably. Worse would be where they cannot do this as they need to go to work...so force themselves into a stressful situation day after day.
2) Given the vaccine efficacy rates, can anyone really see the NHS even approaching overload next winter? If not, then where is the NEED for this approach? If it's not medical (and the BMA seem against it), and it's going beyond what's economically necessary (no need to remove ALL mask-wearing and social-distancing requirements if we just want to open up hospitality etc.), then it's just populism...which is a frankly s
tty way to lead!3) (Most critically) Given what we already know about this virus (and similar viruses), isn't accelerating the spread also accelerating the risk of further mutation into an Echo or Foxtrot variant, potentially (partly or wholly) sidestepping existing immune responses and creating a much bigger problem and many more fatalities...either late-summer/early-Autumn, or (worse) late-Autumn just in time to cause the NHS problems over Winter?
This last one, to me, is the big gamble - we've seen it mutate at least 3x already, and we've seen (in other countries where Delta is still small beer) how restricting the spread of the virus also restricts the ability of any mutation to gain a foothold. So deliberately allowing a virus to run wild on the grounds that "it won't kill that many people"
, while ignoring the very real possibility of adverse mutation seems like a bad mix of:-- Populism
- Optimism
- ...and ignoring medical advice
havoc said:
This last one, to me, is the big gamble - we've seen it mutate at least 3x already, and we've seen (in other countries where Delta is still small beer) how restricting the spread of the virus also restricts the ability of any mutation to gain a foothold. So deliberately allowing a virus to run wild on the grounds that "it won't kill that many people" , while ignoring the very real possibility of adverse mutation seems like a bad mix of:-
- Populism
- Optimism
- ...and ignoring medical advice
There are thousands of different mutations already sequenced. They just don't mention that because it will make it sound like they have no way of controlling it. (Which they don't.), while ignoring the very real possibility of adverse mutation seems like a bad mix of:-- Populism
- Optimism
- ...and ignoring medical advice
Has there been any previous coronavirus that has got more virulent/fatal over time? Or have they all got easier to spread but less deadly, which benefits the virus because it has more hosts and can 'live' longer?
Gassing Station | News, Politics & Economics | Top of Page | What's New | My Stuff