A&E waiting times
Discussion


piquet said:
ok first thing to clear up, the a&e target is 95% leave A&E within 4 hours, we haven't hit it for years, even when we appeared to be doing it in reality we were running at around 92% and used the figures from minor injury units which are often quieter of have an appointment system to boost the average and hit the target. About 2 years ago we got stopped from using that (quite rightly) and then with everything else we've been so far away and there is always massive cheating, back timing etc
The target has good and bad points, A&E being the only place which is always open and the public have direct access to medical care is hit by any other problem in any other part of the NHS be it GP cover, lack of beds, dumping of the elderly, the complete professional disengagement of psychiatrists, staff shortages in the hospital and that's all before you get to staffing in ED. The bad point with it being a quantum target is it means a patient that leaves at 3:59 good, leaves at 4:01 bad
There has been a lot of talk about using the average (mean although you should really use median) is that on an individual level, as a patient you could be there for 24 hours, but it makes no difference. Its a better measure of the stress in the system but does lead to good care. I work in one of the test sites for the new target and for the last 6 months we've had people spending 12-18 hours in the department waiting for a bed for the last 6 months, I went to work at a friends department to help them out this week, i'd forgotten how much better it was with the target. With the target there is pressure to get the patient out, the hospital actively sucks patients out of the department. Without it it is seen as A&Es problem.
There is no clinical evidence for the 4 hour target, it was dreamt up by the Blair government from a focus group The problem with patients staying in A&E is the department gets smaller with each patient, plus the medical staff have to look after patients the same as on the ward as well as processing their own.
Why is it a mess? well the demand keeps going up, when i started we used to see a member of the public every 5 years, we've passed 4 and approaching 3 and of coarse the population has increased significantly during this time. As well as this the ageing and increasingly medical complexity of the population means each elderly patient is so much more complex so sort out.
Before we even think about solving it, we need to realise ll the problems which are hitting us and really this is just some of them, i've tried to group them together.
Outside the NHS
Social care- This is such a mess and needs to be funded properly, sadly this is knock on from the collapse of the family unit, families are split up, all in smaller houses because housing is so expensive which require two incomes for the mortgage, so families can not look after their relatives so the tax payer pays. The sad thing is the family still want to pass on/inherit the value of the house. Maybe some increased in the inheritance threshold if the recipient looks after their relative may help, but i don't know, something has to give. We are swamped with the elderly failing to cope, or having falls and no one to look after them. In the end it needs to be paid for in tax or in time.
Fear of litigation/ health and safety- We get so many people who have been sent it "just to be checked out" firstly it's not how medicine works, just because we don't find anything wrong with you, doesn't mean there isn't. Secondly it's that private gains vs social losses again, people off loading their responsibility to A&E, my sister was the trained first aider for her college, the thing they stressed over and over again was just call an ambulance they didn't actually teach her any more first aid then that and the lesson being you shouldn't be sending them home, always send them to A&E. Just think of the cost of all these ambulances, all the time in ED to the NHS
The 24/7 culture- we all want to have the ability to go food shopping at 3am even if we don't use it, but have the dichotomy of I want to be able to do everything 24/7 but i only want to work monday to friday 9-5. Most of the time this hits the low paid, so making it attractive to work nights or weekends is relatively easy, medical cover is the first place were this becomes difficult not unsurprisingly people are not keen to be forced to work evenings nights, bank holidays and weekends for time and a third and the viability of doing this until people are 68 is nonsense. The target has further fed the demand for evening and night cover why wait until tomorrow when at 8 you can go and be out before midnight. The problem is the antisocial hours are harder and more expensive to staff. The more other people work 24/7 the more problems happen during this time, people are actually pretty safe tucked up in bed.
Drugs and alcohol- everyones whipping boy when it comes to abuse of A&E, but it's not the ones you think who are the problem, the drunk/intoxciated +/- injury and relatively easy and quick to solve. The killer is the chronic patients, the alcoholics and drug addicts, although small in number they create a huge amount work for their number and are very difficult to solve.
Vulnerable adult and children social services- part of our role is to detect the vulnerable and engage social services, after baby P we have been hugely proactive with this and want to make sure it doesn't happen again, my impression of social services its they have learnt nothing from Saville snd Rotherham, i'm guessing because in the end because they weren't prosecuted but it's still going on, and they're still not picking it up
The NHS
Funding- annoying as it is, the NHS needs to get paid for the work it does, if we are required to do more, we need to be paid more in addition to adding the rate of inflation. Controlling the demand or saying what it is we do is the role of the government.
The private sector- The cherry picking of profitable procedures or patients is akin to what the road haulage industry did to the railways with result that lead to the collapse of rail transport. Taking the quick easy procedures on the easy patients proportionally increases the costs on the NHS. In addition the NHS should not be expected to be the trainer or insurer of the private sector. If the private sector is using NHS training then it needs to contribute towards that training cost or train it's own staff. If a patient has private procedure and it goes wrong, then the patient remains a private patient if it's transferred to the NHS, again private gain socialised losses
The feminisation of the workforce- Don't get me wrong, we do not discriminate but the rate of drop outs, parental leave and part time workers is significantly higher in the female workforce. This has then lead to the men who have started to go part time, so you end up with more and more staff who work less and less. Its not helped with the fact it is easy to replace that time you're not working with work which pays better then working for the NHS and this is without the same stress. It is snow balling, it's going to get worse. In emergency medicine training we actively encourage the trainees to go part time as a way of surviving, rather than fix the problem. Sadly once they go part time people almost never come back to full time.
National pay scales- sadly this hits a common theme, because the pay scales are national you can't use the usual market forces to attract people into the hard to fill roles and locations. We end up stupidly short in roles where there is no private practice and have significant anti social working this then feeds into flexible working.
Student loans- it takes a long time to train a doctor, hence unless you come from a wealthy family the debt is massive. When i qualified I was something like 16k in debt and that was significant enough that if i'd known this going in, i wouldn't have gone to medical school. They are now rolling out 100k in debt and with the higher rate of interest have to payback something like 200k. Personally i think as long as you're working for the NHS the NHS should pay your interest, do the equivalent of 30 years full time work for the NHS, the NHS pays the capital.
Mental health- there is a complete failure of mental health provision which results in the patients ending up back in A&E, this sadly falls at the feet of psychiatry who have no interest in providing the cover needed, as a tax payer you are paying for a consultant psychiatrist to be on call at every NHS site, if you ever need them you can never find and they will never come in, except if someone needs sectioning and the sceptic in me is because they are then paid a significant sum for doing it. All of this has been handed off to non medical staff. Whats even worse is despite being looked after by doctors, these doctors refuse to do anything medical for their inpatients, any problem, ambulance to A&E and use them for the medical cover.
Primary care- yes primary care are not providing the cover they should and this feeds back and send the patients to A&E where they will always been seen and the out of hours cover is a disgrace, but they have the same recruitment and work load problems. Its not helped by the GPs been the big fish in their practices, if they phone us for advice we talk to them immediately, when we call them back its 15-20 minutes to get them to come to the phone, that's 15-20 minutes sat on the phone burning time and money
Hospitals
Beds- we just don't have enough, the problem is that they are only efficient if we are always completely full as they cost money to staff even if empty. Unlike a hotel we can't say those who are leaving must be out of a bed by a certain time and no one can come to A&E until 2 hours later. The number of beds we need is pretty easy to calculate, most number of patients who have ever been kept in overnight - least number of patients sent home in one day + most number of patients admitted in one day. Sadly this gives a bed occupancy rate of 85% or lower, most of us are running in excess of 95% hence there just isn't the room and the patients over flow into A&E
IT- the NHS it is awful, we have multiple different systems all with different passwords which change at different frequencies so i spend maybe 30 minutes a day logging on to system or waiting for the system to respond. Sadly the IT staff are those not good enough to get a better paying job elsewhere. Then there is the desire to collect data, as a result about half my day is spent entering data, i'm not a typist ( a quick read of this should confirm that) you turn up too find yet another form, yet another data set had been added all of this takes time to enter and that's time i'm not seeing people.
5/7 vs 7/7- The reality is most of the hospital shuts down at the weekend, you only have to look at the car parks to realise this, it would mean paying people more and properly for the time, but the hospital needs to be fully running 7/7 outpatients should run at weekends, all the services should run. It would cost more but it's 1/3 more work that could be done on the same infrastructure. Trust me MRI scanners do not need to sleep at night and have the weekends off.
Long term planning- There is almost no planning beyond 5 years and nothing beyond 10, this means the actual hospital is never replaced, its rebuilt over and over again, we need to realise that buildings have a finite life and plan for how we are going to replace them, where they will go next and then write the buildings off over the lifespan of them
ok i'll shut up now, but if there is something specific you want to know just ask, sadly most of this boils down to a lack of funds, yes some people need their butts kicking, but most of this can be fixed with money sadly and most of it is caused by trying to run it on the cheap. Healthcare is expensive but like cars, reliable cheap fast, you can only ever have two of the three.
Great post 100% accurate (based on my 30 year experience) saved me a lot if typing!The target has good and bad points, A&E being the only place which is always open and the public have direct access to medical care is hit by any other problem in any other part of the NHS be it GP cover, lack of beds, dumping of the elderly, the complete professional disengagement of psychiatrists, staff shortages in the hospital and that's all before you get to staffing in ED. The bad point with it being a quantum target is it means a patient that leaves at 3:59 good, leaves at 4:01 bad
There has been a lot of talk about using the average (mean although you should really use median) is that on an individual level, as a patient you could be there for 24 hours, but it makes no difference. Its a better measure of the stress in the system but does lead to good care. I work in one of the test sites for the new target and for the last 6 months we've had people spending 12-18 hours in the department waiting for a bed for the last 6 months, I went to work at a friends department to help them out this week, i'd forgotten how much better it was with the target. With the target there is pressure to get the patient out, the hospital actively sucks patients out of the department. Without it it is seen as A&Es problem.
There is no clinical evidence for the 4 hour target, it was dreamt up by the Blair government from a focus group The problem with patients staying in A&E is the department gets smaller with each patient, plus the medical staff have to look after patients the same as on the ward as well as processing their own.
Why is it a mess? well the demand keeps going up, when i started we used to see a member of the public every 5 years, we've passed 4 and approaching 3 and of coarse the population has increased significantly during this time. As well as this the ageing and increasingly medical complexity of the population means each elderly patient is so much more complex so sort out.
Before we even think about solving it, we need to realise ll the problems which are hitting us and really this is just some of them, i've tried to group them together.
Outside the NHS
Social care- This is such a mess and needs to be funded properly, sadly this is knock on from the collapse of the family unit, families are split up, all in smaller houses because housing is so expensive which require two incomes for the mortgage, so families can not look after their relatives so the tax payer pays. The sad thing is the family still want to pass on/inherit the value of the house. Maybe some increased in the inheritance threshold if the recipient looks after their relative may help, but i don't know, something has to give. We are swamped with the elderly failing to cope, or having falls and no one to look after them. In the end it needs to be paid for in tax or in time.
Fear of litigation/ health and safety- We get so many people who have been sent it "just to be checked out" firstly it's not how medicine works, just because we don't find anything wrong with you, doesn't mean there isn't. Secondly it's that private gains vs social losses again, people off loading their responsibility to A&E, my sister was the trained first aider for her college, the thing they stressed over and over again was just call an ambulance they didn't actually teach her any more first aid then that and the lesson being you shouldn't be sending them home, always send them to A&E. Just think of the cost of all these ambulances, all the time in ED to the NHS
The 24/7 culture- we all want to have the ability to go food shopping at 3am even if we don't use it, but have the dichotomy of I want to be able to do everything 24/7 but i only want to work monday to friday 9-5. Most of the time this hits the low paid, so making it attractive to work nights or weekends is relatively easy, medical cover is the first place were this becomes difficult not unsurprisingly people are not keen to be forced to work evenings nights, bank holidays and weekends for time and a third and the viability of doing this until people are 68 is nonsense. The target has further fed the demand for evening and night cover why wait until tomorrow when at 8 you can go and be out before midnight. The problem is the antisocial hours are harder and more expensive to staff. The more other people work 24/7 the more problems happen during this time, people are actually pretty safe tucked up in bed.
Drugs and alcohol- everyones whipping boy when it comes to abuse of A&E, but it's not the ones you think who are the problem, the drunk/intoxciated +/- injury and relatively easy and quick to solve. The killer is the chronic patients, the alcoholics and drug addicts, although small in number they create a huge amount work for their number and are very difficult to solve.
Vulnerable adult and children social services- part of our role is to detect the vulnerable and engage social services, after baby P we have been hugely proactive with this and want to make sure it doesn't happen again, my impression of social services its they have learnt nothing from Saville snd Rotherham, i'm guessing because in the end because they weren't prosecuted but it's still going on, and they're still not picking it up
The NHS
Funding- annoying as it is, the NHS needs to get paid for the work it does, if we are required to do more, we need to be paid more in addition to adding the rate of inflation. Controlling the demand or saying what it is we do is the role of the government.
The private sector- The cherry picking of profitable procedures or patients is akin to what the road haulage industry did to the railways with result that lead to the collapse of rail transport. Taking the quick easy procedures on the easy patients proportionally increases the costs on the NHS. In addition the NHS should not be expected to be the trainer or insurer of the private sector. If the private sector is using NHS training then it needs to contribute towards that training cost or train it's own staff. If a patient has private procedure and it goes wrong, then the patient remains a private patient if it's transferred to the NHS, again private gain socialised losses
The feminisation of the workforce- Don't get me wrong, we do not discriminate but the rate of drop outs, parental leave and part time workers is significantly higher in the female workforce. This has then lead to the men who have started to go part time, so you end up with more and more staff who work less and less. Its not helped with the fact it is easy to replace that time you're not working with work which pays better then working for the NHS and this is without the same stress. It is snow balling, it's going to get worse. In emergency medicine training we actively encourage the trainees to go part time as a way of surviving, rather than fix the problem. Sadly once they go part time people almost never come back to full time.
National pay scales- sadly this hits a common theme, because the pay scales are national you can't use the usual market forces to attract people into the hard to fill roles and locations. We end up stupidly short in roles where there is no private practice and have significant anti social working this then feeds into flexible working.
Student loans- it takes a long time to train a doctor, hence unless you come from a wealthy family the debt is massive. When i qualified I was something like 16k in debt and that was significant enough that if i'd known this going in, i wouldn't have gone to medical school. They are now rolling out 100k in debt and with the higher rate of interest have to payback something like 200k. Personally i think as long as you're working for the NHS the NHS should pay your interest, do the equivalent of 30 years full time work for the NHS, the NHS pays the capital.
Mental health- there is a complete failure of mental health provision which results in the patients ending up back in A&E, this sadly falls at the feet of psychiatry who have no interest in providing the cover needed, as a tax payer you are paying for a consultant psychiatrist to be on call at every NHS site, if you ever need them you can never find and they will never come in, except if someone needs sectioning and the sceptic in me is because they are then paid a significant sum for doing it. All of this has been handed off to non medical staff. Whats even worse is despite being looked after by doctors, these doctors refuse to do anything medical for their inpatients, any problem, ambulance to A&E and use them for the medical cover.
Primary care- yes primary care are not providing the cover they should and this feeds back and send the patients to A&E where they will always been seen and the out of hours cover is a disgrace, but they have the same recruitment and work load problems. Its not helped by the GPs been the big fish in their practices, if they phone us for advice we talk to them immediately, when we call them back its 15-20 minutes to get them to come to the phone, that's 15-20 minutes sat on the phone burning time and money
Hospitals
Beds- we just don't have enough, the problem is that they are only efficient if we are always completely full as they cost money to staff even if empty. Unlike a hotel we can't say those who are leaving must be out of a bed by a certain time and no one can come to A&E until 2 hours later. The number of beds we need is pretty easy to calculate, most number of patients who have ever been kept in overnight - least number of patients sent home in one day + most number of patients admitted in one day. Sadly this gives a bed occupancy rate of 85% or lower, most of us are running in excess of 95% hence there just isn't the room and the patients over flow into A&E
IT- the NHS it is awful, we have multiple different systems all with different passwords which change at different frequencies so i spend maybe 30 minutes a day logging on to system or waiting for the system to respond. Sadly the IT staff are those not good enough to get a better paying job elsewhere. Then there is the desire to collect data, as a result about half my day is spent entering data, i'm not a typist ( a quick read of this should confirm that) you turn up too find yet another form, yet another data set had been added all of this takes time to enter and that's time i'm not seeing people.
5/7 vs 7/7- The reality is most of the hospital shuts down at the weekend, you only have to look at the car parks to realise this, it would mean paying people more and properly for the time, but the hospital needs to be fully running 7/7 outpatients should run at weekends, all the services should run. It would cost more but it's 1/3 more work that could be done on the same infrastructure. Trust me MRI scanners do not need to sleep at night and have the weekends off.
Long term planning- There is almost no planning beyond 5 years and nothing beyond 10, this means the actual hospital is never replaced, its rebuilt over and over again, we need to realise that buildings have a finite life and plan for how we are going to replace them, where they will go next and then write the buildings off over the lifespan of them
ok i'll shut up now, but if there is something specific you want to know just ask, sadly most of this boils down to a lack of funds, yes some people need their butts kicking, but most of this can be fixed with money sadly and most of it is caused by trying to run it on the cheap. Healthcare is expensive but like cars, reliable cheap fast, you can only ever have two of the three.
Edited by piquet on Thursday 16th January 11:45
Esceptico said:
anonymous said:
[redacted]
Yes certain newspapers do like to go on about low paid migrants and seem to forget all the ones with good jobs.It’s numbers of people .. simple
As mothers ruin said it services in the UK need a complete review
It was me that said you have two choices and it’s true
Ignore the problem or fix it
I’d imagine we’ll end up with a typical fudge which will solve nothing
Esceptico said:
The vast majority of those migrants will be working so helping generate revenue for UK companies (so should be adding to corporation tax paid) and of course they will be consuming (VAT) and paying personal taxes. Why haven’t those additional taxes been used to fund the additional services that a growing population needs? I suppose it can’t be the Tories fault as they haven’t been in government for a decade...
and yet despite that the public finances are only just returning towards balance after years of controlling spending. If all of those who have come in their millions are such a fiscal boon why isn't there the spare cash to pay for all the schools, hospitals, transport infrastructure JagLover said:
and yet despite that the public finances are only just returning towards balance after years of controlling spending. If all of those who have come in their millions are such a fiscal boon why isn't there the spare cash to pay for all the schools, hospitals, transport infrastructure
Keeping boomers onside mostly. amongst other things, It was spent on submarines, pensions and Norther Ireland bungs.Esceptico said:
The vast majority of those migrants will be working so helping generate revenue for UK companies (so should be adding to corporation tax paid) and of course they will be consuming (VAT) and paying personal taxes. Why haven’t those additional taxes been used to fund the additional services that a growing population needs? I suppose it can’t be the Tories fault as they haven’t been in government for a decade...
Citation needed... Please don't rely on mean analysis, when you're claiming a very clear and specific distribution curve.
sawman said:
piquet said:
ok first thing to clear up, the a&e target is 95% leave A&E within 4 hours, we haven't hit it for years, even when we appeared to be doing it in reality we were running at around 92% and used the figures from minor injury units which are often quieter of have an appointment system to boost the average and hit the target. About 2 years ago we got stopped from using that (quite rightly) and then with everything else we've been so far away and there is always massive cheating, back timing etc
The target has good and bad points, A&E being the only place which is always open and the public have direct access to medical care is hit by any other problem in any other part of the NHS be it GP cover, lack of beds, dumping of the elderly, the complete professional disengagement of psychiatrists, staff shortages in the hospital and that's all before you get to staffing in ED. The bad point with it being a quantum target is it means a patient that leaves at 3:59 good, leaves at 4:01 bad
There has been a lot of talk about using the average (mean although you should really use median) is that on an individual level, as a patient you could be there for 24 hours, but it makes no difference. Its a better measure of the stress in the system but does lead to good care. I work in one of the test sites for the new target and for the last 6 months we've had people spending 12-18 hours in the department waiting for a bed for the last 6 months, I went to work at a friends department to help them out this week, i'd forgotten how much better it was with the target. With the target there is pressure to get the patient out, the hospital actively sucks patients out of the department. Without it it is seen as A&Es problem.
There is no clinical evidence for the 4 hour target, it was dreamt up by the Blair government from a focus group The problem with patients staying in A&E is the department gets smaller with each patient, plus the medical staff have to look after patients the same as on the ward as well as processing their own.
Why is it a mess? well the demand keeps going up, when i started we used to see a member of the public every 5 years, we've passed 4 and approaching 3 and of coarse the population has increased significantly during this time. As well as this the ageing and increasingly medical complexity of the population means each elderly patient is so much more complex so sort out.
Before we even think about solving it, we need to realise ll the problems which are hitting us and really this is just some of them, i've tried to group them together.
Outside the NHS
Social care- This is such a mess and needs to be funded properly, sadly this is knock on from the collapse of the family unit, families are split up, all in smaller houses because housing is so expensive which require two incomes for the mortgage, so families can not look after their relatives so the tax payer pays. The sad thing is the family still want to pass on/inherit the value of the house. Maybe some increased in the inheritance threshold if the recipient looks after their relative may help, but i don't know, something has to give. We are swamped with the elderly failing to cope, or having falls and no one to look after them. In the end it needs to be paid for in tax or in time.
Fear of litigation/ health and safety- We get so many people who have been sent it "just to be checked out" firstly it's not how medicine works, just because we don't find anything wrong with you, doesn't mean there isn't. Secondly it's that private gains vs social losses again, people off loading their responsibility to A&E, my sister was the trained first aider for her college, the thing they stressed over and over again was just call an ambulance they didn't actually teach her any more first aid then that and the lesson being you shouldn't be sending them home, always send them to A&E. Just think of the cost of all these ambulances, all the time in ED to the NHS
The 24/7 culture- we all want to have the ability to go food shopping at 3am even if we don't use it, but have the dichotomy of I want to be able to do everything 24/7 but i only want to work monday to friday 9-5. Most of the time this hits the low paid, so making it attractive to work nights or weekends is relatively easy, medical cover is the first place were this becomes difficult not unsurprisingly people are not keen to be forced to work evenings nights, bank holidays and weekends for time and a third and the viability of doing this until people are 68 is nonsense. The target has further fed the demand for evening and night cover why wait until tomorrow when at 8 you can go and be out before midnight. The problem is the antisocial hours are harder and more expensive to staff. The more other people work 24/7 the more problems happen during this time, people are actually pretty safe tucked up in bed.
Drugs and alcohol- everyones whipping boy when it comes to abuse of A&E, but it's not the ones you think who are the problem, the drunk/intoxciated +/- injury and relatively easy and quick to solve. The killer is the chronic patients, the alcoholics and drug addicts, although small in number they create a huge amount work for their number and are very difficult to solve.
Vulnerable adult and children social services- part of our role is to detect the vulnerable and engage social services, after baby P we have been hugely proactive with this and want to make sure it doesn't happen again, my impression of social services its they have learnt nothing from Saville snd Rotherham, i'm guessing because in the end because they weren't prosecuted but it's still going on, and they're still not picking it up
The NHS
Funding- annoying as it is, the NHS needs to get paid for the work it does, if we are required to do more, we need to be paid more in addition to adding the rate of inflation. Controlling the demand or saying what it is we do is the role of the government.
The private sector- The cherry picking of profitable procedures or patients is akin to what the road haulage industry did to the railways with result that lead to the collapse of rail transport. Taking the quick easy procedures on the easy patients proportionally increases the costs on the NHS. In addition the NHS should not be expected to be the trainer or insurer of the private sector. If the private sector is using NHS training then it needs to contribute towards that training cost or train it's own staff. If a patient has private procedure and it goes wrong, then the patient remains a private patient if it's transferred to the NHS, again private gain socialised losses
The feminisation of the workforce- Don't get me wrong, we do not discriminate but the rate of drop outs, parental leave and part time workers is significantly higher in the female workforce. This has then lead to the men who have started to go part time, so you end up with more and more staff who work less and less. Its not helped with the fact it is easy to replace that time you're not working with work which pays better then working for the NHS and this is without the same stress. It is snow balling, it's going to get worse. In emergency medicine training we actively encourage the trainees to go part time as a way of surviving, rather than fix the problem. Sadly once they go part time people almost never come back to full time.
National pay scales- sadly this hits a common theme, because the pay scales are national you can't use the usual market forces to attract people into the hard to fill roles and locations. We end up stupidly short in roles where there is no private practice and have significant anti social working this then feeds into flexible working.
Student loans- it takes a long time to train a doctor, hence unless you come from a wealthy family the debt is massive. When i qualified I was something like 16k in debt and that was significant enough that if i'd known this going in, i wouldn't have gone to medical school. They are now rolling out 100k in debt and with the higher rate of interest have to payback something like 200k. Personally i think as long as you're working for the NHS the NHS should pay your interest, do the equivalent of 30 years full time work for the NHS, the NHS pays the capital.
Mental health- there is a complete failure of mental health provision which results in the patients ending up back in A&E, this sadly falls at the feet of psychiatry who have no interest in providing the cover needed, as a tax payer you are paying for a consultant psychiatrist to be on call at every NHS site, if you ever need them you can never find and they will never come in, except if someone needs sectioning and the sceptic in me is because they are then paid a significant sum for doing it. All of this has been handed off to non medical staff. Whats even worse is despite being looked after by doctors, these doctors refuse to do anything medical for their inpatients, any problem, ambulance to A&E and use them for the medical cover.
Primary care- yes primary care are not providing the cover they should and this feeds back and send the patients to A&E where they will always been seen and the out of hours cover is a disgrace, but they have the same recruitment and work load problems. Its not helped by the GPs been the big fish in their practices, if they phone us for advice we talk to them immediately, when we call them back its 15-20 minutes to get them to come to the phone, that's 15-20 minutes sat on the phone burning time and money
Hospitals
Beds- we just don't have enough, the problem is that they are only efficient if we are always completely full as they cost money to staff even if empty. Unlike a hotel we can't say those who are leaving must be out of a bed by a certain time and no one can come to A&E until 2 hours later. The number of beds we need is pretty easy to calculate, most number of patients who have ever been kept in overnight - least number of patients sent home in one day + most number of patients admitted in one day. Sadly this gives a bed occupancy rate of 85% or lower, most of us are running in excess of 95% hence there just isn't the room and the patients over flow into A&E
IT- the NHS it is awful, we have multiple different systems all with different passwords which change at different frequencies so i spend maybe 30 minutes a day logging on to system or waiting for the system to respond. Sadly the IT staff are those not good enough to get a better paying job elsewhere. Then there is the desire to collect data, as a result about half my day is spent entering data, i'm not a typist ( a quick read of this should confirm that) you turn up too find yet another form, yet another data set had been added all of this takes time to enter and that's time i'm not seeing people.
5/7 vs 7/7- The reality is most of the hospital shuts down at the weekend, you only have to look at the car parks to realise this, it would mean paying people more and properly for the time, but the hospital needs to be fully running 7/7 outpatients should run at weekends, all the services should run. It would cost more but it's 1/3 more work that could be done on the same infrastructure. Trust me MRI scanners do not need to sleep at night and have the weekends off.
Long term planning- There is almost no planning beyond 5 years and nothing beyond 10, this means the actual hospital is never replaced, its rebuilt over and over again, we need to realise that buildings have a finite life and plan for how we are going to replace them, where they will go next and then write the buildings off over the lifespan of them
ok i'll shut up now, but if there is something specific you want to know just ask, sadly most of this boils down to a lack of funds, yes some people need their butts kicking, but most of this can be fixed with money sadly and most of it is caused by trying to run it on the cheap. Healthcare is expensive but like cars, reliable cheap fast, you can only ever have two of the three.
Great post 100% accurate (based on my 30 year experience) saved me a lot if typing!The target has good and bad points, A&E being the only place which is always open and the public have direct access to medical care is hit by any other problem in any other part of the NHS be it GP cover, lack of beds, dumping of the elderly, the complete professional disengagement of psychiatrists, staff shortages in the hospital and that's all before you get to staffing in ED. The bad point with it being a quantum target is it means a patient that leaves at 3:59 good, leaves at 4:01 bad
There has been a lot of talk about using the average (mean although you should really use median) is that on an individual level, as a patient you could be there for 24 hours, but it makes no difference. Its a better measure of the stress in the system but does lead to good care. I work in one of the test sites for the new target and for the last 6 months we've had people spending 12-18 hours in the department waiting for a bed for the last 6 months, I went to work at a friends department to help them out this week, i'd forgotten how much better it was with the target. With the target there is pressure to get the patient out, the hospital actively sucks patients out of the department. Without it it is seen as A&Es problem.
There is no clinical evidence for the 4 hour target, it was dreamt up by the Blair government from a focus group The problem with patients staying in A&E is the department gets smaller with each patient, plus the medical staff have to look after patients the same as on the ward as well as processing their own.
Why is it a mess? well the demand keeps going up, when i started we used to see a member of the public every 5 years, we've passed 4 and approaching 3 and of coarse the population has increased significantly during this time. As well as this the ageing and increasingly medical complexity of the population means each elderly patient is so much more complex so sort out.
Before we even think about solving it, we need to realise ll the problems which are hitting us and really this is just some of them, i've tried to group them together.
Outside the NHS
Social care- This is such a mess and needs to be funded properly, sadly this is knock on from the collapse of the family unit, families are split up, all in smaller houses because housing is so expensive which require two incomes for the mortgage, so families can not look after their relatives so the tax payer pays. The sad thing is the family still want to pass on/inherit the value of the house. Maybe some increased in the inheritance threshold if the recipient looks after their relative may help, but i don't know, something has to give. We are swamped with the elderly failing to cope, or having falls and no one to look after them. In the end it needs to be paid for in tax or in time.
Fear of litigation/ health and safety- We get so many people who have been sent it "just to be checked out" firstly it's not how medicine works, just because we don't find anything wrong with you, doesn't mean there isn't. Secondly it's that private gains vs social losses again, people off loading their responsibility to A&E, my sister was the trained first aider for her college, the thing they stressed over and over again was just call an ambulance they didn't actually teach her any more first aid then that and the lesson being you shouldn't be sending them home, always send them to A&E. Just think of the cost of all these ambulances, all the time in ED to the NHS
The 24/7 culture- we all want to have the ability to go food shopping at 3am even if we don't use it, but have the dichotomy of I want to be able to do everything 24/7 but i only want to work monday to friday 9-5. Most of the time this hits the low paid, so making it attractive to work nights or weekends is relatively easy, medical cover is the first place were this becomes difficult not unsurprisingly people are not keen to be forced to work evenings nights, bank holidays and weekends for time and a third and the viability of doing this until people are 68 is nonsense. The target has further fed the demand for evening and night cover why wait until tomorrow when at 8 you can go and be out before midnight. The problem is the antisocial hours are harder and more expensive to staff. The more other people work 24/7 the more problems happen during this time, people are actually pretty safe tucked up in bed.
Drugs and alcohol- everyones whipping boy when it comes to abuse of A&E, but it's not the ones you think who are the problem, the drunk/intoxciated +/- injury and relatively easy and quick to solve. The killer is the chronic patients, the alcoholics and drug addicts, although small in number they create a huge amount work for their number and are very difficult to solve.
Vulnerable adult and children social services- part of our role is to detect the vulnerable and engage social services, after baby P we have been hugely proactive with this and want to make sure it doesn't happen again, my impression of social services its they have learnt nothing from Saville snd Rotherham, i'm guessing because in the end because they weren't prosecuted but it's still going on, and they're still not picking it up
The NHS
Funding- annoying as it is, the NHS needs to get paid for the work it does, if we are required to do more, we need to be paid more in addition to adding the rate of inflation. Controlling the demand or saying what it is we do is the role of the government.
The private sector- The cherry picking of profitable procedures or patients is akin to what the road haulage industry did to the railways with result that lead to the collapse of rail transport. Taking the quick easy procedures on the easy patients proportionally increases the costs on the NHS. In addition the NHS should not be expected to be the trainer or insurer of the private sector. If the private sector is using NHS training then it needs to contribute towards that training cost or train it's own staff. If a patient has private procedure and it goes wrong, then the patient remains a private patient if it's transferred to the NHS, again private gain socialised losses
The feminisation of the workforce- Don't get me wrong, we do not discriminate but the rate of drop outs, parental leave and part time workers is significantly higher in the female workforce. This has then lead to the men who have started to go part time, so you end up with more and more staff who work less and less. Its not helped with the fact it is easy to replace that time you're not working with work which pays better then working for the NHS and this is without the same stress. It is snow balling, it's going to get worse. In emergency medicine training we actively encourage the trainees to go part time as a way of surviving, rather than fix the problem. Sadly once they go part time people almost never come back to full time.
National pay scales- sadly this hits a common theme, because the pay scales are national you can't use the usual market forces to attract people into the hard to fill roles and locations. We end up stupidly short in roles where there is no private practice and have significant anti social working this then feeds into flexible working.
Student loans- it takes a long time to train a doctor, hence unless you come from a wealthy family the debt is massive. When i qualified I was something like 16k in debt and that was significant enough that if i'd known this going in, i wouldn't have gone to medical school. They are now rolling out 100k in debt and with the higher rate of interest have to payback something like 200k. Personally i think as long as you're working for the NHS the NHS should pay your interest, do the equivalent of 30 years full time work for the NHS, the NHS pays the capital.
Mental health- there is a complete failure of mental health provision which results in the patients ending up back in A&E, this sadly falls at the feet of psychiatry who have no interest in providing the cover needed, as a tax payer you are paying for a consultant psychiatrist to be on call at every NHS site, if you ever need them you can never find and they will never come in, except if someone needs sectioning and the sceptic in me is because they are then paid a significant sum for doing it. All of this has been handed off to non medical staff. Whats even worse is despite being looked after by doctors, these doctors refuse to do anything medical for their inpatients, any problem, ambulance to A&E and use them for the medical cover.
Primary care- yes primary care are not providing the cover they should and this feeds back and send the patients to A&E where they will always been seen and the out of hours cover is a disgrace, but they have the same recruitment and work load problems. Its not helped by the GPs been the big fish in their practices, if they phone us for advice we talk to them immediately, when we call them back its 15-20 minutes to get them to come to the phone, that's 15-20 minutes sat on the phone burning time and money
Hospitals
Beds- we just don't have enough, the problem is that they are only efficient if we are always completely full as they cost money to staff even if empty. Unlike a hotel we can't say those who are leaving must be out of a bed by a certain time and no one can come to A&E until 2 hours later. The number of beds we need is pretty easy to calculate, most number of patients who have ever been kept in overnight - least number of patients sent home in one day + most number of patients admitted in one day. Sadly this gives a bed occupancy rate of 85% or lower, most of us are running in excess of 95% hence there just isn't the room and the patients over flow into A&E
IT- the NHS it is awful, we have multiple different systems all with different passwords which change at different frequencies so i spend maybe 30 minutes a day logging on to system or waiting for the system to respond. Sadly the IT staff are those not good enough to get a better paying job elsewhere. Then there is the desire to collect data, as a result about half my day is spent entering data, i'm not a typist ( a quick read of this should confirm that) you turn up too find yet another form, yet another data set had been added all of this takes time to enter and that's time i'm not seeing people.
5/7 vs 7/7- The reality is most of the hospital shuts down at the weekend, you only have to look at the car parks to realise this, it would mean paying people more and properly for the time, but the hospital needs to be fully running 7/7 outpatients should run at weekends, all the services should run. It would cost more but it's 1/3 more work that could be done on the same infrastructure. Trust me MRI scanners do not need to sleep at night and have the weekends off.
Long term planning- There is almost no planning beyond 5 years and nothing beyond 10, this means the actual hospital is never replaced, its rebuilt over and over again, we need to realise that buildings have a finite life and plan for how we are going to replace them, where they will go next and then write the buildings off over the lifespan of them
ok i'll shut up now, but if there is something specific you want to know just ask, sadly most of this boils down to a lack of funds, yes some people need their butts kicking, but most of this can be fixed with money sadly and most of it is caused by trying to run it on the cheap. Healthcare is expensive but like cars, reliable cheap fast, you can only ever have two of the three.
Edited by piquet on Thursday 16th January 11:45
You should both go and talk to Shami Chakrabarti as I'm not sure her views on what the employees think entirely match with the above.
I've luckily only ever had 2 experiences of having to go to hospital.
Once 20 years ago as a teenager after being ran over by a large 4x4 with bull bars on the front.
On arrival I was put in a wheel chair and was eventually seen to 4.5 hours later.
More recently my partner had a suspected torn ligament whilst out skiing in Bulgaria, on our arrival back to the UK we went to A&E and same scenario, put in a wheelchair on arrival and seen to around 4 hours later.
Once 20 years ago as a teenager after being ran over by a large 4x4 with bull bars on the front.
On arrival I was put in a wheel chair and was eventually seen to 4.5 hours later.
More recently my partner had a suspected torn ligament whilst out skiing in Bulgaria, on our arrival back to the UK we went to A&E and same scenario, put in a wheelchair on arrival and seen to around 4 hours later.
DaveH23 said:
More recently my partner had a suspected torn ligament whilst out skiing in Bulgaria, on our arrival back to the UK we went to A&E and same scenario, put in a wheelchair on arrival and seen to around 4 hours later.
Sorry to hear about your partnerIf you arrive in AE with an injury that you sustained a few days earlier which isnt life threatening then how long do you think should be a reasonable time to wait?
numtumfutunch said:
DaveH23 said:
More recently my partner had a suspected torn ligament whilst out skiing in Bulgaria, on our arrival back to the UK we went to A&E and same scenario, put in a wheelchair on arrival and seen to around 4 hours later.
Sorry to hear about your partnerIf you arrive in AE with an injury that you sustained a few days earlier which isnt life threatening then how long do you think should be a reasonable time to wait?
My post was to illustrate that long waiting times is nothing new. There was a 20 year gap between the 2 incidents above yet the waiting times where the same.
Perhaps what I'm getting that is that people go on like the NHS waiting times are getting worse but in my experience they have been the way they are for quite a long time.
loafer123 said:
I didn’t realise until yesterday that the 4 hour target they use is to be seen and leave the A&E (through discharge or admission) and not the waiting time to be seen.
Yep. Triage tends to happen in minutes, not hours... It's a classic gamed metric that's meaningless - as Seddon showed. If you want to meet it as a department, triage everyone pronto. Deal with the emergencies pronto.
Everyone else? Just focus all resources on those hitting the three and a half hour threshold - then rapidly either clear them out, or shunt them onto a ward.
Just like state secondaries focusing all their attentions on those "just" missing the requisite C grades (or whatever number they are now) rather than everyone. The fly on the wall school docs (the one with the stuttering kid and the teacher who played music through headphones for him springs to mind) made that focus of resources to meet targets very clear...
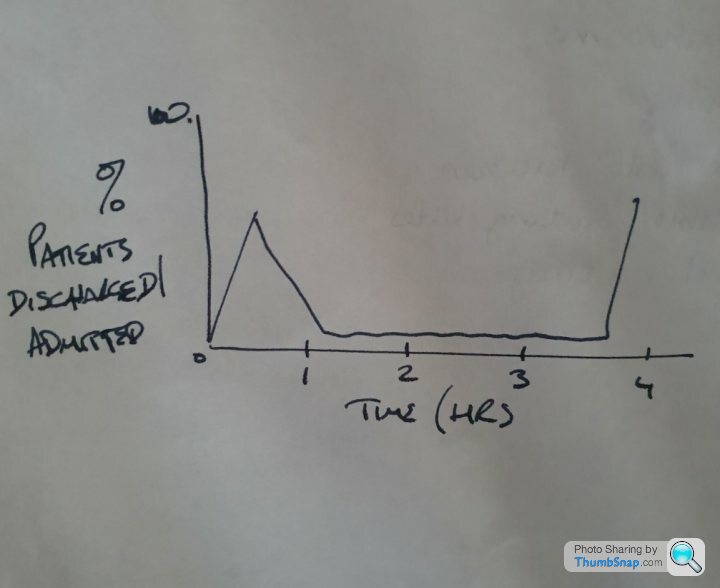
Desperately trying to show the gif which plotted a histogram distribution of patient waiting times in A&E that absolutely demonstrates my point regarding how the target completely f ked the system, and the vast majority of patients...
ked the system, and the vast majority of patients...
In the meantime, this is quite interesting - see the allocation of resources purely to manage the target, rather than actually managing the system and patients properly:
https://www.google.com/url?sa=t&source=web&...
ked the system, and the vast majority of patients...In the meantime, this is quite interesting - see the allocation of resources purely to manage the target, rather than actually managing the system and patients properly:
https://www.google.com/url?sa=t&source=web&...
DaveH23 said:
Don't apologise I agree wholeheartedly with you, people arriving via blue light or with anything suspected of being life-threatening should absolutely take presidence.
He wasn't apologising. He has nothing to apologise for. He was sympathising with you."people arriving via blue light or with anything suspected of being life-threatening should absolutely take presidence"
That is how it works. It is the system. It is called triage. It is designed to be that way.
https://en.wikipedia.org/wiki/Triage
Sway said:
Yep. Triage tends to happen in minutes, not hours...
It's a classic gamed metric that's meaningless - as Seddon showed. If you want to meet it as a department, triage everyone pronto. Deal with the emergencies pronto.
Everyone else? Just focus all resources on those hitting the three and a half hour threshold - then rapidly either clear them out, or shunt them onto a ward.
Just like state secondaries focusing all their attentions on those "just" missing the requisite C grades (or whatever number they are now) rather than everyone. The fly on the wall school docs (the one with the stuttering kid and the teacher who played music through headphones for him springs to mind) made that focus of resources to meet targets very clear...
It isn’t just triage;It's a classic gamed metric that's meaningless - as Seddon showed. If you want to meet it as a department, triage everyone pronto. Deal with the emergencies pronto.
Everyone else? Just focus all resources on those hitting the three and a half hour threshold - then rapidly either clear them out, or shunt them onto a ward.
Just like state secondaries focusing all their attentions on those "just" missing the requisite C grades (or whatever number they are now) rather than everyone. The fly on the wall school docs (the one with the stuttering kid and the teacher who played music through headphones for him springs to mind) made that focus of resources to meet targets very clear...
“ The four-hour standard measures the total time patients spend in A&E rather than the time patients spend ‘waiting’ for treatment to begin. The waiting time clock ‘starts’ from the time that the patient arrives in A&E and stops when they leave the department to be admitted, transferred to another provider (for example, where more specialist clinical care is needed) or discharged. For patients arriving by ambulance, the clock starts when the patient is handed over from the ambulance staff to hospital staff or 15 minutes after the ambulance arrives at A&E (whichever is earlier).“
loafer123 said:
Sway said:
Yep. Triage tends to happen in minutes, not hours...
It's a classic gamed metric that's meaningless - as Seddon showed. If you want to meet it as a department, triage everyone pronto. Deal with the emergencies pronto.
Everyone else? Just focus all resources on those hitting the three and a half hour threshold - then rapidly either clear them out, or shunt them onto a ward.
Just like state secondaries focusing all their attentions on those "just" missing the requisite C grades (or whatever number they are now) rather than everyone. The fly on the wall school docs (the one with the stuttering kid and the teacher who played music through headphones for him springs to mind) made that focus of resources to meet targets very clear...
It isn’t just triage;It's a classic gamed metric that's meaningless - as Seddon showed. If you want to meet it as a department, triage everyone pronto. Deal with the emergencies pronto.
Everyone else? Just focus all resources on those hitting the three and a half hour threshold - then rapidly either clear them out, or shunt them onto a ward.
Just like state secondaries focusing all their attentions on those "just" missing the requisite C grades (or whatever number they are now) rather than everyone. The fly on the wall school docs (the one with the stuttering kid and the teacher who played music through headphones for him springs to mind) made that focus of resources to meet targets very clear...
“ The four-hour standard measures the total time patients spend in A&E rather than the time patients spend ‘waiting’ for treatment to begin. The waiting time clock ‘starts’ from the time that the patient arrives in A&E and stops when they leave the department to be admitted, transferred to another provider (for example, where more specialist clinical care is needed) or discharged. For patients arriving by ambulance, the clock starts when the patient is handed over from the ambulance staff to hospital staff or 15 minutes after the ambulance arrives at A&E (whichever is earlier).“
What I meant, was effectively you had "two" overall waiting times - either "superfast" for the emergencies, or "a couple of minutes inside 4 hours to be discharged/admitted" for everyone else.
Effectively, no one was discharged/admitted between minutes 60 and 220.
Something like this, massively "fag packet" histogram of waiting times to discharge/admittance I've quickly scribbled:

Last time I was in A&E was a few months ago now, Mrs. had been having stabbing pains in her abdomen a few times which would usually go away after a few hours, GP didn't do anything about it after multiple visits, so during the latest episode, took her to A&E waited about 5/6 hours to see a Dr, to be told it was suspected gallstones after about 5 minutes diagnosis, and to be scheduled in for an MRI in a couple days time, then had to have her gall bladder out a few weeks later. Could have avoided the whole thing if the GP had referred her for an MRI after the first or even 2nd time she spoke to them about it, but they didn't, The waiting room was full the entire time we were there, complete with the obvious known drunk time waster who was there for another timewasting session and a sleep and had to be escorted out by security.
I'm currently going through the same with my GP about my back problems; "how long has it been hurting"; "about 8 years"; "ohh, here's a prescription for co-codomol, come back in 2 weeks if it's not any better", next time it gets really bad, I'm not even going to bother with the GP, just going to go waste myself and A&E's time, currently managing myself with over the counter medicines, with pain and restricted movement still present.
I'm currently going through the same with my GP about my back problems; "how long has it been hurting"; "about 8 years"; "ohh, here's a prescription for co-codomol, come back in 2 weeks if it's not any better", next time it gets really bad, I'm not even going to bother with the GP, just going to go waste myself and A&E's time, currently managing myself with over the counter medicines, with pain and restricted movement still present.
Gassing Station | News, Politics & Economics | Top of Page | What's New | My Stuff